

- UA
- EN
Омега-3
Джек Норріс, сертифікований дієтолог
Зміст
Рівні довголанцюгових омега-3 жирних кислот у крові вегетаріанців
Добавки ALA призводять до незначного підвищення рівня DHA у крові
Відсотки EPA та DHA корелюють між плазмою та тканинами серця, але не тканинами мозку
Менше споживання омега-6 пов’язане з вищим вмістом EPA та DHA в сироватці
Додаток B: Еволюційні аргументи на користь дієтичних потреб у DHA
Основна інформація
Омега-3 жири важливі для довгострокового здоров’я серця та мозку, але містяться в обмеженій кількості рослинних продуктів. Волоські горіхи, ріпакова олія, насіння льону та лляна олія, насіння чіа, насіння конопель та перилова олія мають високий вміст омега-3.
Рецепт пудингу з насіння чіа
Смачний спосіб отримувати щоденну дозу омега-3 — пудинг із насіння чіа, який можна їсти на сніданок або як десерт.
Інгредієнти
1+3/4 склянки несолодкого рослинного молока (або підсолодженого рослинного молока — тоді виключіть підсолоджувач із інгредієнтів нижче)
1-2 столові ложки підсолоджувача (наприклад, цукру або кленового сиропу)
1/2 чашки насіння чіа
1/2 до 1 чайної ложки ванільного екстракту (необов'язково)
Спосіб приготування
У мисці збийте всі інгредієнти.
Охолодіть кілька годин і перемішайте перед вживанням.
Ще краще подавати з начинками, такими як фрукти, арахісова паста або шоколадна крихта.
Зберігати в холодильнику.

Інший варіант — тримати банку конопель або меленого насіння льону в холодильнику, щоб посипати ними їжу протягом дня. Насіння легко поєднується з будь-якою їжею.
Референтні норми споживання ALA
У таблиці нижче наведено референтні добові норми споживання (DRI) для необхідного омега-3 жиру, альфа-ліноленової кислоти (ALA).
Рослинні джерела ALA
Додаткові поради
Питання про те, чи потрібно веганам робити щось додатково, крім отримання рекомендованої норми, є суперечливим (і детально обговорюється нижче).
Для особливої обережності вегани можуть робити одну додаткову річ з наступного:
Споживайте додатково 2000 мг ALA на день, використовуючи продукти, наведені в таблиці вище.
Приймайте добавки 200-300 мг DHA на день.
Ваша добавка DHA може містити EPA, але це необов’язково, якщо ви споживаєте рекомендовану кількість ALA. Ми не маємо позиції щодо конкретних брендів добавок DHA.
Завелика кількість омега-3 може призвести до кровотечі та синців. Якщо ви схильні до кровотечі чи синяків, проконсультуйтеся з лікарем, перш ніж значно збільшити споживання омега-3.
Дивіться нижче наші рекомендації під час вагітності, годування груддю та для немовлят.
Льон
Якщо насіння льону не подрібнити, воно не засвоїться [Austria, 2008]. Їх можна подрібнити в блендері (найкраще це працює з великою кількістю) або кавомолці, а потім зберігати в морозилці. Меленим насінням льону можна посипати пластівці або використовувати його для приготування випічки.
Є певні докази того, що люди віком від 45 років не засвоюють олію з меленого насіння льону так само добре, як із олії з насіння льону [Patenaude, 2009]. Одне дослідження, яке показало це, тривало лише чотири тижні та використовувало 6 г ALA на день. За менших кількостей і протягом тривалішого періоду різниця може бути незначною, але це не перевірялося.
Приготування лляної олії пошкоджує ALA, але її можна додавати до теплої їжі, наприклад тостів.
Лляна олія повинна зберігатися в холодильнику.
Лляна олія не дуже смачна. Деякі люди використовують лляну олію зі смаком кориці, таблетки або кладуть її на тости чи салати, щоб замаскувати смак.
Дослідження омега-3 жирних кислот у рослинних дієтах
Є два запитання щодо вегетаріанців і омега-3: чи мають вегетаріанці негативні наслідки для здоров’я від того, що не вживають рибу, і чи варто вегетаріанцям вживати добавки омега-3, які містяться в рибі (EPA та DHA)? Хоча багато досліджень показали, що у вегетаріанців і веганів рівень EPA і DHA в крові нижчий, ніж у тих, хто їсть рибу, швидка відповідь на ці запитання полягає в тому, що немає достатніх доказів, щоб зробити висновок про те, що низькі рівні мають негативні наслідки для здоров’я.
Далі ми обговорюватимемо аргументи та дослідження навколо цього питання.
Довідкова інформація про Омега-3
Для цілей нашого обговорення є чотири важливі омега-3 жирні кислоти:
Альфа-ліноленова кислота (АЛК, ALA) • Коротколанцюгова (18 атомів вуглецю) омега-3 жирна кислота. Міститься у невеликих кількостях у м’ясі тварин, у дуже малих кількостях — у різноманітних продуктах рослинного походження та у відносно великих кількостях — у сої, волоських горіхах, ріпаковій олії, насінні льону та лляній олії, олії насіння коноплі, рижієвій олії, периловій олії та насінні чіа. Організм людини не може виробляти власну ALA; її необхідно отримувати з дієти.
Ейкозапентаєнова кислота (ЕПК, EPA) • Довголанцюгова (20 атомів вуглецю) омега-3 жирна кислота. Міститься в основному в жирній рибі, у невеликих кількостях — в яйцях і в дуже невеликих кількостях — у морських водоростях, які можна концентрувати в добавках. Деякі EPA перетворюються на ейкозаноїди 3 серії, які можуть зменшити згортання крові, запалення, артеріальний тиск і холестерин. Організм людини може виробляти EPA з ALA і, можливо, з DHA.
Докозапентаєнова кислота (ДПК, DPA) • Довголанцюгова (22 атомів вуглецю) жирна кислота. Існує як омега-3, так і омега-6 версія DPA. Версія DPA омега-3 є посередником між EPA і DHA.
Докозагексаєнова кислота (ДГК, DHA) • Довголанцюгова (22 атомів вуглецю) омега-3 жирна кислота. Міститься в основному в жирній рибі, у невеликих кількостях — в яйцях і в дуже невеликих кількостях — у морських водоростях, які можна концентрувати і використовувати в вигляді добавок. DHA є основним компонентом сірої речовини мозку, а також міститься в серці, сітківці, яєчках, спермі та клітинних мембранах. Організм може перетворювати EPA в DHA.
У таблиці нижче показано шляхи перетворення омега-3 і омега-6 жирних кислот. На діаграмі D6D — це фермент, який перетворює ALA і LA (лінолева кислота, омега-6) в інші жири.

Прогляньте відео нижче із чудовим оглядом омега-3 жирних кислот від дослідника омега-3, доктора Річарда Базінета з Університету Торонто (2021).
[[VIDEO https://www.youtube.com/watch?v=fPkx8U9f-dI ]]
Споживання незамінних жирних кислот веганами
Інститут медицини США вважає, що люди віком від 1 року мають потребу в двох жирних кислотах: альфа-ліноленовій кислоті (ALA) і лінолевій кислоті (LA). Однак [Burdge (2022)] повідомляє, що явний дефіцит ALA ніколи не був досліджений окремо від дефіциту LA та жиророзчинних вітамінів у дорослих людей, щоб чітко продемонструвати, що ALA є незамінною жирною кислотою.
У таблиці нижче наведено середні зважені значення досліджень, що вимірюють споживання ALA веганами. Розрахунки та посилання — в Електронній таблиці ALA Intakes.
[Всесвітня організація охорони здоров’я та Продовольча та сільськогосподарська організація (2010)] рекомендують споживання LA від 2,5% до 9% калорій, стверджуючи, що менша кількість запобігає дефіциту, а більша межа діапазону знижує ризик серцевих захворювань.
Хоча вегани, які не забезпечують джерел ALA, як правило, мають високе співвідношення омега-6 до омега-3 жирів, їхній відсоток калорій для LA становить 5,1% [Pinto, 2017, United Kingdom], 7,3% [Allès, 2017, France], 8,5% [Kornsteiner, 2008, Austria], і 9,3% [Rizzo, 2013, USA], — цілком у межах діапазону, рекомендованого ВОЗ.
Рівні довголанцюгових омега-3 жирних кислот у крові вегетаріанців
Резюме: відмінності в рівнях довголанцюгових омега-3 у крові між веганами, лактоововегетаріанцями та всеїдними не є очевидно фізіологічно значущими, особливо щодо всеїдних, які регулярно не їдять рибу. Рівень DHA в еритроцитах вегетаріанців і веганів становить приблизно 72-75% від рівня всеїдних людей, але неясно, чи має це клінічне значення.
Немає стандартизованого методу вимірювання омега-3 жирних кислот: ніхто не знає, які рівні жирних кислот у будь-якому середовищі представляють дефіцитний, здоровий або оптимальний рівень. Можливо навіть, що рівень жирних кислот у крові мало впливає на рівень омега-3 жирних кислот в організмі. Мета цього розділу — визначити, чи справді у веганів нижчий рівень довголанцюгових омега-3 жирних кислот у крові, ніж у всеїдних. Ранні дослідження показали, що вегани мають нижчий рівень EPA і DHA в крові, але ці дослідження проводилися на малій кількості людей; новіші дослідження майже не показали різниці.
Станом на початок 2022 року ми відстежили 27 досліджень, у яких вимірювали рівень омега-3 жирних кислот у вегетаріанців. Ми перелічуємо ці дослідження та їх вимірювання у вкладці "Перехресні дослідження" нашої електронної таблиці про дослідження омега-3.
Спосіб визначення омега-3 у цих дослідженнях суттєво відрізняється.
Жирні кислоти можна виміряти в різних компонентах плазми, як-от фосфоліпіди, тригліцериди або ефіри холестерину. Жирні кислоти також можна виміряти в жировій тканині, тромбоцитах або еритроцитах. Оскільки еритроцити живуть 120 днів, жирні кислоти еритроцитів можуть бути точнішим довгостроковим відображенням рівня омега-3.
У плазмі омега-3 зазвичай вимірюється як відсоток від загальної кількості жирних кислот, але [Welch et al. (2010)] вимірювали омега-3 як концентрацію їх у плазмі, а [Rosell et al. (2005)] надали дані для розрахунку цієї концентрації. Концентрації можуть бути точнішим відображенням запасів омега-3 в організмі, оскільки вони являють собою абсолютну, а не відносну кількість.
DPA — це довголанцюгова омега-3 жирна кислота, яка є посередником між EPA та DHA. Ми наголошуємо на дослідженнях, які включали DPA у свої вимірювання, оскільки DPA представляє значну частку довголанцюгових омега-3, яких вегани перетворили з ALA і які потенційно можуть бути перетворені на DHA.
На графіку нижче показано всі вимірювання, які порівнювали загальні рівні довголанцюгових омега-3 (EPA+DPA+DHA) у вегетаріанців або веганів із всеїдними. Він включає вимірювання відсотків і концентрацій для кожного середовища. Незважаючи на значний збіг між групами дієт, окремі дослідження загалом показують, що всеїдні мають більший рівень довголанцюгових омега-3, ніж вегани, причому відмінності є статистично значущими.
 у вегетаріанців або веганів із всеїдними людьми")
На графіках нижче порівнюються лише рівні EPA або DHA у веганів і вегетаріанців у всіх дослідженнях, які вимірювали EPA або DHA.


Можливо, найважливішим показником є дані про омега-3 в еритроцитах, показані на графіку нижче.

Із цих досліджень важко зробити багато висновків щодо рівня довголанцюгових омега-3 у веганів, враховуючи, що вимірювання не стандартизовані, недостатньо зрозумілі та суттєво перехрещуються. Можливо, точніший спосіб оцінити ці дані — одночасно протиставити порівняння вегетаріанців пропорційно до всеїдних у тих же дослідженнях, і також пропорційно до кількості людей у кожній групі дієти, обмежуючи вимірювання одним показником на досліджувану популяцію.
Щоб отримати найточнішу картину порівняння рівня довголанцюгових омега-3 у крові веганів і всеїдних людей, ми вирішили відкалібрувати вимірювання, створивши співвідношення між рівнями веганів і всеїдних, а не використовувати абсолютне значення. Для цього ми просто поділили рівні веганів на рівні всеїдних людей.
Наприклад, дослідження [Kornsteiner et al.] виявило, що відсоток EPA+DPA+DHA від загальної кількості жирних кислот у еритроцитах становить 1,96% для веганів і 3,34% для всеїдних. Дослідження [Li et al.] виявило, що відсоток EPA+DPA+DHA від загальної кількості жирних кислот у плазмі становить 3,6% для веганів і 5,5% для всеїдних. Ми не знаємо, чи зможемо ми порівняти відсоток жирних кислот у еритроцитах із жирними кислотами в плазмі, але ми можемо порівняти співвідношення довголанцюгових омега-3 у веганів та всеїдних в обох дослідженнях, яке становило 0,59 у Kornsteiner та ін. і 0,65 у Li та ін.
Потім ми можемо помножити ці два співвідношення на кількість веганів у відповідному дослідженні, розділити на загальну кількість веганів в обох дослідженнях — і отримати середньозважене співвідношення довголанцюгових омега-3 для веганів і всеїдних в обох дослідженнях. Зваживши всі дослідження таким чином, ми можемо отримати найточнішу картину порівняння рівня довголанцюгових омега-3 жирних кислот у крові веганів і всеїдних.
Більшість досліджень вимірювали омега-3 як відсоток від загальної кількості жирних кислот; щоб бути максимально послідовними, ми зважили відсоток омега-3 відносно загальної кількості жирних кислот, а не концентрацію омега-3 для тих досліджень, які вимірювали обидва цих показника. Для досліджень із кількома вимірюваннями ми вибрали показники в такому порядку: еритроцити, плазма, тромбоцити та жирова тканина.
У таблиці нижче показано зважені пропорції омега-3 у вегетаріанців і веганів у порівнянні з всеїдними для всіх досліджень і лише для вимірювання еритроцитів. Розрахунки та посилання є у Крос-секційній вкладці нашої електронної таблиці.
Виходячи з таблиці вище, у веганів зазвичай нижчий рівень довголанцюгових омега-3 у крові, ніж у всеїдних. Оскільки рівні омега-3 у плазмі принаймні частково відображають жирні кислоти, що постачаються з їжею (окремо від відображення здатності організму перетворювати харчові коротколанцюгові омега-3 у довголанцюгові), недивно, що люди, які споживають довголанцюгові омега-3, мають вищі рівні омега-3 у крові.
Вегетаріанці проти споживачів риби
Серед людей, які не приймають довголанцюгові омега-3 жирні кислоти, ті, хто регулярно споживають рибу, будуть єдиною дієтичною групою зі значним джерелом довголанцюгових омега-3. Відповідно до бази даних поживних речовин USDA, середньостатисничне яйце містить близько 2 мг EPA і 16 мг DHA. Це забезпечує лактоововегетаріанців дуже невеликими кількостями харчових EPA та DHA.
Є два дослідження, які вимірювали рівень омега-3 серед споживачів риби [Welch, 2010] [Miles, 2019], але жодне не вимірювало його в еритроцитах. Ми аналізуємо ці дослідження у Вкладці про споживачів риби нашої електронної таблиці Омега-3. Частина 2: Дослідження і підсумовуємо результати у трьох діаграмах нижче. Учасники дослідження не вживали довголанцюгові добавки омега-3.
[Welch, 2010] виміряли концентрацію омега-3 у плазмі крові та розділили всеїдних на групи, які споживали та не споживали рибу. Серед учасників було лише 10 веганів.
Ми об’єднали концентрації довголанцюгових омега-3 у чоловіків і жінок у плазмі крові, щоб порівняти показники веганів із всеїдними, які споживають рибу, і всеїдними, які не споживають рибу. Оскільки веганів було дуже мало, ми також об’єднали лактоововегетаріанців (LOV) із веганами до категорії «вегетаріанців». У наведеній нижче таблиці показано, що лактоововегетаріанці, вегани або об’єднана їхня група мали трохи нижчі рівні порівняно з тими, хто їсть рибу, і однакові або вищі порівняно з тими, хто не їсть рибу.
[Miles, 2019] порівняли відсоток омега-3 жирних кислот у жировій тканині пескетаріанців з іншими дієтичними групами, як показано в таблиці нижче. У вегетаріанців та веганів виявлено нижчий рівень, ніж у всеїдних, і дещо нижчий, ніж у тих, хто споживає рибу. При цьому незрозуміло, який відсоток жирних кислот у жировій тканині; можливо, це не має достатньої клінічної значущості.
Рівні жирних кислот у літніх веганів проти молодих
Вважається, що з віком людям важче перетворювати ALA в EPA та DHA. [Sarter et al. (2015)] виявили, що 69 веганів віком від 60 до 85 років мали рівні EPA+DHA приблизно 4,0% порівняно з приблизно 3,6% у 97 веганів віком від 20 до 59 років (Імовірність для тенденції = 0,009).
Вплив нижчого рівня EPA та DHA на вегетаріанців
Можливою перевагою довголанцюгових омега-3 жирних кислот, особливо EPA, є зниження згортання крові, що захищає від серцевих нападів. Були виявлені деякі відмінності в згортанні крові між вегетаріанцями та всеїдними.
[Mezzano et al. (1999, Chile)], виявили, що вегетаріанці мають значно більше тромбоцитів (242 000 на мкл), ніж невегетаріанці (211 000 на мкл), і менший час кровотечі (4,5 проти 7,3 хв), що може збільшити ризик серцево-судинних подій. У подальшому дослідженні [Mezzano et al., 2000, Chile)] вегетаріанцям давали 700 мг EPA і 700 мг DHA протягом 8 тижнів. У результаті рівень EPA зріс із 0,2 до 1,8%, а DHA — із 1,1 до 3,0%. Деякі фактори згортання крові змінилися, але час кровотечі залишився меншим і становив 5-1/2 хвилини.
[Sanders and Roshani (1992, United Kingdom)] виявили, що один із восьми параметрів агрегації тромбоцитів у чоловіків-веганів, але не у жінок, відрізнявся від показників у невегетаріанців. Тривалість кровотечі була однаковою.
[Pinto et al. (2017, United Kingdom)] порівняли варіабельність серцевого ритму між групою з 23 дорослих веганів і 24 всеїдних. Низька варіабельність серцевого ритму відображає знижену здатність серця реагувати на фізіологічні потреби організму та пов’язана з підвищеним ризиком серцевих захворювань. Як і очікувалося, у веганів були нижчі концентрації DHA і EPA як в еритроцитах, так і в плазмі. У веганів була більша варіабельність серцевого ритму протягом 24-годинного періоду, при цьому денна варіабельність серцевого ритму була нижчою, а частота серцевих скорочень більшою. Клінічне значення цих знахідок не до кінця зрозуміле.
Таким чином, результати трьох досліджень, які вивчали серцево-судинні маркери, неоднозначні.
Щодо когнітивних функцій, у дослідженні британської смертності [Appleby et al. (2002)] виявили, що вегетаріанці мають вищий ризик смерті (ледь статистично значущий) від психічних і неврологічних захворювань (DRR: 2,21, CI: 1,02–4,78).
Навпаки, у нещодавному звіті EPIC-Oxford [Appleby, 2016] виявили, що смертність вегетаріанців від психічних і поведінкових розладів статистично не відрізняється від смерті невегетаріанців (HR: 1,22, CI: 0,78–1,91). Також у звіті Adventist Health Study-2 [Orlich, 2013, USA] не виявили різниці в смертності від неврологічних захворювань між вегетаріанцями та невегетаріанцями (HR: 0,93, CI: 0,67-1,29); Пескетаріанці та напіввегетаріанці були включені до вегетаріанської категорії, тому результати не можна екстраполювати на вегетаріанців, які не вживають рибу.
Перетворення ALA в EPA і DHA
Вимірювання відсотка загального вмісту жирних кислот, таких як EPA та DHA, у крові, як правило, вважається маркером рівня омега-3. Відповідно до цього припущення, більший відсоток загального вмісту жирних кислот у крові відображає вищі та оптимальніші кількості в тканинах, які використовують омега-3. А також коли процентний вміст крові змінюється через зміни в раціоні, рівні в тканинах реагують подібним чином.
У цьому розділі ми розглядаємо ці припущення. Докази щодо ферментів перетворення омега-3 у тканинах і зниження перетворення омега-3 у відповідь на збільшення постачання омега-3 з їжею свідчать про те, що організм може регулювати перетворення омега-3 жирних кислот у тканинах незалежно від відсоткового вмісту в крові.
Є докази того, що високе споживання EPA та DHA збільшить їхній відсоток як у крові, так і в тканинах, але незрозуміло, чи потрібні вищі відсотки для кращого здоров’я. Ми оцінюємо ці докази в розділах Вплив нижчого рівня EPA та DHA на вегетаріанців і Омега-3 і хронічні захворювання.
Добавки ALA призводять до незначного підвищення рівня DHA у крові
У Таблиці випробувань ALA наведено декілька клінічних випробувань, включаючи всі відомі нам випробування за участю вегетаріанців, які досліджують, чи збільшення харчових ALA згодом збільшує відсоток довголанцюгових омега-3 у крові. Зміни загального вмісту жирних кислот у вигляді довголанцюгових омега-3 демонструють широкі варіації без чіткої закономірності; деякі навіть виявили зниження рівня DHA. У середньому рівень EPA+DPA+DHA збільшився на 43,5%, тоді як рівень DHA збільшився лише на 4,6%.
Можна з упевненістю сказати, що прийом добавок ALA навряд чи суттєво збільшить відсоток жирних кислот у крові, як-от DHA, у більшості дорослих.
Відсотки EPA та DHA корелюють між плазмою та тканинами серця, але не тканинами мозку
Резюме: На підставі обмежених, здебільшого перехресних даних, існує надійна кореляція між відсотками EPA+DHA у крові та тканинах серця людини, але не тканинах мозку чи спермі.
Дослідження добавок ALA призводять до дуже незначного збільшення DHA в крові, але скільки є доказів того, що це відображає нездатність організму перетворювати ALA в DHA для використання тканинами?
Основне питання полягає в тому, наскільки рівень омега-3 жирних кислот у крові зазвичай корелює з рівнем у тканинах без будь-яких змін у харчуванні? Досліджувати вміст омега-3 в тканинах живих людей складно. В електронній таблиці Кореляції тканин ми перераховуємо кореляцію між процентним вмістом омега-3 в крові та тканинах як у людей, так і у тварин. Нижче наведено підсумок результатів.
[Harris et al. (2004)] виміряли кореляцію між відсотком EPA+DHA в еритроцитах і відсотком EPA+DHA в серцях 20 пацієнтів після трансплантації серця, які проходили звичайну біопсію серця. 13 із них отримували багато EPA і DHA. У дослідженні виявили статистично значущу, сильну кореляцію (Кореляція = 0,82, Імовірність ≤ 0,0001).
[Harris et al. (2004)] також провели втручання: пацієнти з трансплантацією серця (n=25) з низьким споживанням EPA+DHA отримували 1000 мг EPA+DHA протягом 6 місяців. У цих пацієнтів були слабші кореляції між еритроцитами та EPA+DHA серця на початковому рівні (Кореляція = 0,47, P = 0,031). Вимірювання після втручання показали, що відсоток EPA+DHA збільшився в плазмі, еритроцитах, тканинах серця та щік; кореляція між еритроцитами та EPA+DHA серця залишилася незмінною (Кореляція = 0,47, P = 0,06).
[Metcalf et al. (2007)] давали ряду пацієнтів ALA (5,8 г на день) або EPA+DHA (6,3 г, ~50% кожному) протягом кількох тижнів на основі графіка операції на серці. Хоча дослідники не перевіряли кореляцію між відсотками омега-3 жирних кислот еритроцитів і серця, відсотки двох цих середовищ були досить подібними та відрізнялися від контрольної групи подібним чином після впробування (див. нашу електронну таблицю про Випробування ALA).
[Cunnane et al. (2012)] провели розтин когнітивно здорових людей і виявили кореляцію між відсотками DHA у фосфатидилетаноламіну плазми та відсотками DHA ділянки кутової звивини мозку (Кореляція = 0,77, P ≤ 0,005). Однак їм не вдалося виявити кореляції між DHA з інших ділянок або перевірити все це у людей з порушеннями когнітивних функцій: «Не спостерігалося суттєвих кореляцій між DHA (% або мг/г) або будь-якими іншими жирними кислотами в інших областях мозку або в групі [хвороби Альцгеймера ] і групах [з легкими когнітивними порушеннями] (дані не вказані)».
[Carver et al. (2001)] провели розтин 58 людей і виявили негативну кореляцію між відсотком DHA в еритроцитах і корі головного мозку людей старше 18 років; ймовірно, ця кореляція не досягає статистичної значущості після поправки Бонферроні для великої кількості перевірених кореляцій.
[Chamorro et al. (2020)] вимірювали відсоток жирних кислот у молодих чоловіків, порівнюючи веганів (розмір вибірки = 34) і всеїдних (розмір вибірки = 33). Дослідники не перевіряли кореляцію між відсотком омега-3 у плазмі або еритроцитах і спермі. Співвідношення відсоткового вмісту EPA в спермі в плазмі та еритроцитах було подібним і становило 0,54, але співвідношення для DPA та DHA не були такими. Дивіться таблицю нижче.
Даних про тварин набагато більше, ніж про людей. У нашій електронній таблиці — Кореляції тканин — перелічено 24 кореляції між відсотками EPA+DHA в крові та тканинах у щурів, свиней і мишей. Сила кореляцій значно змінюється, деякі з кореляцій негативні.
Варто згадати ще одне дослідження на тваринах. [Talahalli et al. (2010)] годували дві групи щурів доцільною кількістю ALA (2,5% і 5,0% калорій). Через 60 днів відсоток жирних кислот у вигляді DHA у мозку щурів, які отримували 2,5% і 5,0% ALA, становив відповідно 9,4% і 10,4% порівняно з 8,3% у контрольній групі (див. таблицю, Talahalli 2010). Це свідчить про те, що додавання ALA збільшило кількість DHA у їхньому мозку.
Одне суттєве застереження для порівняння перетворення омега-3 у щурів, свиней і мишей у людей полягає в тому, що щури, свині та миші зазвичай не мають харчового джерела EPA або DHA і, отже, зазвичай повністю покладаються на перетворення з ALA на будь-який EPA або DHA.
Хоча відсоток довголанцюгових омега-3 жирних кислот у плазмі та еритроцитах іноді корелює з відсотком у тканинах, ця кореляція не послідовна. Можливо, можна розробити математичну модель, яка могла би пояснити велику кількість змінних, які впливають на кореляції, але здається малоймовірним, що буде розроблена модель, яка дасть нам впевненість у прогнозуванні рівня омега-3 у тканинах вегетаріанців.
У Додатку А ми обговорюємо оглядову статтю «Біомаркери рівня DHA», в якій стверджується, що відсотки крові є адекватними маркерами рівня DHA.
Тканини містять ферменти, які перетворюють Омега-3
Два найважливіших ферменти, дельта-5-десатураза і дельта-6-десатураза, перетворюють коротколанцюгові омега-3 і омега-6 жирні кислоти в довголанцюгові версії. Раніше печінка вважалася основним місцем вироблення EPA та DHA для використання периферичними тканинами, але у дослідженнях [Cho et al., 1999a] і [Cho et al., 1999b] було виявлено значну кількість мРНК для ферментів дельта-5 і дельта-6-десатурази в багатьох тканинах людських трупів.
[Cho et al., 1999a] виявили, що найбільше мРНК дельта-5-десатурази в печінці людини, але в серці, мозку та легенях також міститься значна кількість. Дослідники виявили низькі, але помітні рівні в плаценті, скелетних м’язах, нирках і підшлунковій залозі. [Cho et al., 1999b] виявили, що кількість мРНК дельта-6-десатурази в печінці людини порівнюється з тією, що міститься в легенях і серці людини, тоді як у мозку дорослої людини цей рівень у кілька разів перевищує рівень печінки.
[Cho et al., 1999a] зазначають, що експресія цих ферментів може суттєво відрізнятися в окремих людей. Автори припускають, що це може бути пов’язано з віком або, що більш імовірно на їхню думку, з регуляцією ферментів у відповідь на споживання жирних кислот з їжею.
Використовуючи крос-секційні дані на основі відсотка фосфоліпідів плазми, [Welch et al. (2008, United Kingdom)] підрахували, що організми людей, які не їдять рибу (як вегетаріанців, так і всеїдних), перетворюють ALA на довголанцюгові омега-3 приблизно на 22% швидше, ніж ті, хто вживають рибу.
Харчова DHA зменшує перетворення ALA
У серії з трьох досліджень дослідники використовували вуглецевий індикатор для відстеження перетворення дози 700 мг ALA в довголанцюгові омега-3 в крові трьох різних груп людей. Результати наведено в таблиці нижче. Лише жінки (усі з яких були репродуктивного віку) продемонстрували значне перетворення ALA в DHA в крові.
На додаток до базових вимірювань, наведених у таблиці вище, дослідження [Burdge et al. (2003)] включало 8-тижневе втручання на трьох групах літніх чоловіків: контрольній групі (розмір вибірки = 5), групі, у якої щоденне споживання ALA було збільшено зі звичного споживання 1,7 г до 10 г (розмір вибірки = 4), і групі, у якої EPA+DHA було збільшено зі звичного споживання 264 мг до 1,6 г (розмір вибірки = 5). Через 8 тижнів кожній людині дали 700 мг ALA з вуглецевим індикатором і виявили, що перетворення ALA в довголанцюгові омега-3 у групи, яка вживала ALA, не збільшилося, тоді як у групи, яка вживала EPA+DHA, перетворення зменшилося.
[Vermunt et al. (2000)] давали людям ALA, мічену вуглецем, і виявили, що перетворення ALA в EPA, DPA та DHA було набагато активнішим після 9 тижнів дієти з високим вмістом олеїнової кислоти (омега-9) порівняно з дієтою з високим вмістом ALA або EPA+DHA.
Два випробування, згадані вище — [Burdge et al. (2003)] і [Vermunt et al. (2000)] — припускають, що у людей із регулярним надходженням ALA або EPA і DHA відбувається зниження перетворення ALA в довголанцюгові омега-3. Найпростішим поясненням цього зниження є те, що їхні тканини мали достатній рівень довголанцюгових омега-3.
Додатковим доказом ферментативної регуляції внаслідок споживання їжі є дослідження, проведене [Metherel et al. (2019)]. У його межах було проведено рандомізоване контрольоване дослідження з використанням міченої вуглецем DHA. Хоча рівні EPA в плазмі зросли, це не було пов’язано з перетворенням DHA в EPA, що свідчить про те, що надходження DHA в їжу призвело до зниження регуляції перетворення EPA в DHA.
Дані дослідження [Burdge and Wootton’s (2002)] показали нерівномірний розподіл омега-3 жирних кислот серед різних компонентів ліпідів плазми (ефіри холестерину, фосфатидилхолін, тригліцериди та неестерифіковані жирні кислоти). Дослідники припустили, що ефіри холестерину в плазмі діють як довгострокове джерело ALA в кровообігу, яке може забезпечити тканини, що містять активні шляхи десатурації та елонгації (мозок, серце та скелетні м’язи), постійним джерелом ALA для перетворення в EPA, DPA та DHA, тоді як тканини з низькою експресією цих ферментів, як-от нирки та підшлункова залоза, можуть залежати від постачання попередньо сформованих EPA, DPA та DHA.
Менше споживання омега-6 пов’язане з вищим вмістом EPA та DHA в сироватці
Традиційний спосіб, яким вегетаріанців спонукали підвищити рівень EPA і DHA в крові, полягає в збільшенні споживання ALA і зменшенні омега-6 жирної кислоти, лінолевої кислоти (LA). Це пояснюється тим, що ферменти, які перетворюють ALA в EPA і DHA, також перетворюють омега-6 жирні кислоти, і існує конкуренція за ці ферменти. Деякі докази цієї теорії отримано з клінічних випробувань [Liou et al. (2007, Canada)], які виявили, що збільшення споживання LA призвело до зниження відсотка EPA у плазмових фосфоліпідах
Більшість рослинних олій мають високий вміст омега-6, і вегетаріанці, як правило, отримують їх у великій кількості. [Sanders and Younger (1981, United Kingdom] виявили дієтичне співвідношення омега-6 до омега-3, яке дорівнювало 16 для веганів і 6 для м’ясоїдів. [Sanders and Roshanai (1992, United Kingdom)] виявили, що дієтичне співвідношення для чоловіків-веганів становить 15,8, для чоловіків-всеїдних — 10,2, для жінок-веганок — 18,3 і для жінок, які їдять м’ясо, — 8,2.
Немає жодних клінічних випробувань, які би збільшували споживання ALA вегетаріанцями, одночасно зменшуючи споживання LA, щоб побачити, як це впливає на рівні EPA та DHA в крові.
[Salvador et al. (2019, Spain)] аналізували показники у 55 веганів і 49 лактоововегетаріанців і виявили, що ті, у кого співвідношення омега-6 до омега-3 в сироватці крові ≤ 10, мали вищий відсоток сироваткових EPA і DHA, ніж ті, у кого співвідношення від 10 до 20 або >20 (EPA: 0,60%, 0,27% і 0,23%; DHA: 2,90%, 1,91% і 1,19% відповідно). Споживання насіння льону один раз на день, особливо 2 або більше разів на день, було пов’язано з набагато вищим відсотком сироваткової ALA (~0,5% проти ~0,7% і 1,5% відповідно), але не з вищим відсотком EPA або DHA.
Згідно з обмеженими дослідженнями, зниження споживання LA може підвищити рівень довголанцюгових омега-3 в крові, але невідомо, чи впливає це на тканини та чи приносить користь для здоров’я.
Продукти з низьким співвідношенням омега-6 до омега-3
Наразі проведені дослідження вказують на те, що вегетаріанці з низьким співвідношенням омега-6 до омега-3 в їжі, як правило, мають вищі рівні EPA і DHA в крові. Через це доцільно, додаючи ALA до раціону, вибирати продукти, які також суттєво не збільшують споживання омега-6, — вони перераховані у таблиці нижче.
Прийом добавок DHA вегетаріанцями
Дослідження послідовно показують, що прийом вегетаріанцями і веганами добавок DHA з водоростей підвищує відсоток DHA у їхній крові [Sanders, 2009] [Geppert, 2006] [Wu, 2006] [Conquer, 1996] [Conquer, 1997]. Дослідження також показують, що прийом добавок EPA і DHA збільшує відсоток EPA і DHA у вегетаріанців [Sarter, 2015] [Mezzano, 2000].
Риба містить приблизно вдвічі більше DHA, ніж EPA [Kris-Etherton, 2009], тому люди, які споживають рибу, нерідко отримують більше DHA, ніж EPA. [Conquer and Holub (1996, Canada)] показали збільшення EPA на 11-12% після 6 тижнів прийому 1620 мг DHA у вегетаріанців.
При прийомі добавки DHA рівень EPA також підвищується на невеликий відсоток. Використовуючи вуглецевий індикатор, [Brossard et al. (1996, France)] виявили 1,4% перетворення DHA в EPA у трьох людей, які отримували одну дозу 123 мг DHA протягом 20 годин. На противагу цьому [Metherel et al. (2019, Canada)] провели рандомізоване контрольоване дослідження з використанням DHA, що містить мічений вуглець, і не виявили перетворення на EPA. Вони дійшли висновку, що «збільшення рівня EPA в плазмі після прийому добавки DHA у людей відбувається не через ретроконверсію, а внаслідок уповільненого метаболізму та/або накопичення EPA в плазмі».
Рекомендації щодо омега-3 для веганів
Підведемо підсумок обґрунтування наших рекомендацій: виявляється, що якщо вегани отримують рекомендовану норму ALA, у них має бути достатній рівень EPA. Для обережності ми рекомендуємо або збільшити споживання ALA, або додати добавку DHA. Перегляньте нашу статтю Щоденні потреби, щоб отримати конкретні рекомендації.
В інтернеті є багато веганських добавок DHA та EPA. Ми не можемо оцінити, чи той чи інший виробник кращий за інший.
Вегетаріанство, вагітність, годування та немовлята
У цьому розділі наведено наші рекомендації щодо омега-3 для вегетаріанців і веганів, а потім обговорюється поточний стан досліджень.
Резюме та рекомендації
В США та Канаді рекомендації з харчування (DRI) не наполягають на добавках DHA під час вагітності або годування груддю. Вони рекомендують додаткові 300 мг ALA під час вагітності (загалом 1,4 г/день) і додаткові 200 мг ALA під час годування груддю (загалом 1,3 г/день). Їхні рекомендації для немовлят, яких не годують грудьми, стосуються дитячої суміші з 500 мг загальної кількості омега-3 (ALA, EPA та DHA) на день [National Institutes of Health, 2022].
Проте низка організацій перевизначили рекомендовану добову норму (DRI), спеціально рекомендувавши DHA для широкої громадськості під час вагітності та/або годування груддю, включаючи Міжнародне товариство з вивчення жирних кислот і ліпідів (International Society for the Study of Fatty Acids and Lipids, ISSFAL) і Американську академію педіатрії (American Academy of Pediatrics, AAP).
Останній Кокрейнівський аналіз рандомізованих контрольованих досліджень виявив користь добавок DHA у запобіганні ранніх передчасних пологів серед зовні здорових вагітних жінок [Middleton, 2018]. Метою наших рекомендацій у VeganHealth є запобігання дефіциту поживних речовин, а не лікування хвороб.
Висновок про те, що DHA знижує ризик невеликого відсотка передчасних пологів, можливо, пов’язаний з терапевтичним ефектом DHA, а не з виправленням дефіциту поживних речовин. Якщо це так, то дотримання DRI для ALA може запобігти дефіциту омега-3 під час вагітності та годування груддю, але без додаткових досліджень доцільно проявити обережність.
Наші рекомендації щодо вагітності, годування груддю та немовлят:
Дієта матері під час вагітності
Дотримуйтесь рекомендованої норми ALA — 1,4 г на день (див. Щоденні потреби).
Вживайте добавку з 300-600 мг DHA на день [Carlson, 2013] [Harris, 2015].
Дієта матері під час годування
Дотримуйтесь рекомендованої норми для ALA — 1,3 г на день (див. Щоденні потреби).
Докази не є переконливими для добавок DHA, але деякі організації рекомендують щонайменше 200 мг на день [Koletzko, 2007] [Meek and Noble, 2022].
Діти на штучному вигодовуванні
Використовуйте дитячу суміш з 500 мг загальної кількості омега-3 (ALA, EPA та DHA) на день; EPA і DHA не потрібні, якщо є 500 мг ALA.
Діти, які харчуються тільки твердою їжею
Дотримуйтесь рекомендованої норми DRI для ALA (кількості та джерела — див. Щоденні потреби).
Дослідження вагітних і годуючих веганок
[Ureta-Velasco et al. (2023, Spain)] порівняли грудне молоко 20 вегетаріанок (включаючи 11 веганок) із молоком всеїдних. Автори описують своє дослідження як одне з найповніших доступних досліджень завдяки наявності 5-денного звіту з харчування, кількох зразків молока від кожної учасниці та вимірювання рівня поживних речовин у плазмі. Проте дослідження було проведено для визначення якості грудного молока вегетаріанок для донорських цілей, і молоко оброблялося та зберігалося так само, як і донорське грудне молоко; автори сказали, що через це результати не можна застосовувати до грудного молока, яким безпосередньо годують немовлят.
Споживання ALA становило 1,58 г/день для всеїдних жінок і 2,24 г/день для матерів-вегетаріанок. Серед вегетаріанської групи 30% вживали добавки омега-3 під час вагітності та 35% вживали їх під час годування груддю. Загальне споживання EPA плюс DHA, включно з добавками, становило 0,53 г/день для всеїдних жінок і 0,14 г/день для вегетаріанок. Як показано на діаграмі нижче, DHA в еритроцитах, плазмі та грудному молоці вегетаріанок було значно менше.
Автори пишуть:
“Однак ми не вважаємо це причиною для виключення жінок-вегетаріанок і веганок як донорів молока. По-перше, споживання та рівні DHA в жіночому молоці сильно відрізняються в різних країнах. Дійсно, було зафіксовано навіть нижчі рівні споживання та вмісту, ніж у нашої групи вегетаріанок, як у розвинених країнах, так і в країнах, що розвиваються. Насправді кілька досліджень [донорського жіночого молока] в Північній Америці виявили, що рівні DHA були подібні або навіть нижчі, ніж у нашої групи. По-друге, оскільки додавання DHA жінкам, які годують, постійно демонструє підвищення концентрації DHA у грудному молоці, здається доцільною стратегією рекомендувати додавання DHA з олії водоростей вегетаріанкам і веганкам, які хочуть стати донорками молока.”
[Specker et al. (1987, USA)] порівняли вміст жиру в грудному молоці 7 невегетаріанок із 12 жінками, які дотримувалися макробіотичної дієти (в основному веганської, іноді з тваринними продуктами, включаючи морепродукти). Відсоток DHA до всіх жирів у грудному молоці жінок був подібним (0,27% для жінокна макробіотичній дієті і 0,29% для невегетаріанок).
[Reddy and Sanders (1994, United Kingdom)] виміряли рівень DHA в пуповині 32 немовлят, народжених від матерів-вегетаріанок індійського походження, що проживають у Північному Лондоні, і порівняли їх із всеїдними матерями. У вегетаріанок виявили нижчий відсоток фосфоліпідів пуповинної плазми DHA (4,0% проти 5,8%) і фосфоліпідів пуповинної артерії (4,1% проти 5,8%). Діти вегетаріанок індійського походження народжувалися з меншою масою тіла, меншим зростом та меншою окружністю голови, але не було жодного зв’язку між цими параметрами та відсотковим вмістом DHA у їхній плазмі крові або фосфоліпідах пуповинної артерії.
[Reddy and Sanders (1994, United Kingdom)] також виміряли відсоток DHA відносно всіх жирів у грудному молоці 19 веганок (0,14%), 5 вегетаріанок (0,30%) і 21 всеїдної жінки (0,37%).
[Perrin et al. (2018, USA)] виявили, що ALA у грудному молоці було значно більше у веганок (2,1%), ніж у вегетаріанок (1,4%) і всеїдних жінок (1,2%). Дослідники не виявили статистично значущих відмінностей між рівнями DHA у 26 веганок (0,14%), 22 вегетаріанок (0,17%) і 26 всеїдних жінок (0,18%). DHA було неможливо виявити в 14,9% зразків; не було різниці в поширеності невизначуваних зразків між групами дієти.
Автори зазначають:
“У двох незалежних оглядах концентрації DHA у грудному молоці в усьому світі повідомлялося про середні показники 0,32–0,37%, при цьому концентрації в популяції США часто становили 0,20% або нижче, що близько до наших висновків. Тоді як використання добавки DHA добре підтверджується в літературі як спосіб збільшення DHA в грудному молоці, менше однієї третини веганів у нашому дослідженні повідомили про використання добавок DHA. Подібним чином, споживання риби було низьким, лише 3/26 (11,5%) всеїдних і 0/22 (0,0%) вегетаріанців повідомили про частіше, ніж щотижневе, споживання.”
Оскільки доношені діти віком до 3 тижнів можуть перетворювати ALA в DHA [Sauerwald, 1996], незрозуміло, чи має низький відсоток DHA у веганському грудному молоці достатню фізіологічну значущість.
Дослідження харчових добавок омега-3 під час вагітності, годування груддю та для немовлят
Десятки клінічних випробувань оцінювали вплив добавок DHA на розвиток дитини. У деяких дослідженнях DHA давали безпосередньо немовлятам, а в інших їхнім вагітним або годуючим матерям.
Є два великих систематичних огляди на цю тему:
Омега-3 жирні кислоти та здоров'я матері та дитини: оновлений систематичний огляд [Newberry et al., 2016], підготовлений для Агентства досліджень і якості охорони здоров’я (Agency for Healthcare Research and Quality, AHRQ) Міністерства охорони здоров’я та соціальних служб США. Цей понад 800-сторінковий звіт містить аналіз 95 рандомізованих контрольованих досліджень і 48 обсерваційних досліджень.
Додавання омега-3 жирних кислот під час вагітності [Middleton, et al., 2018], систематичний огляд Кокрейнівської бази даних. Цей понад 400-сторінковий звіт містить аналіз 70 рандомізованих контрольованих досліджень.
Висновки дещо різні, особливо щодо ризику передчасних пологів.
У звіті AHRQ [Newberry et al., 2016] встановили, що доказів достатньо, щоб зробити висновок про низьку або помірну силу для таких результатів:
Добавки DHA збільшили тривалість вагітності, але не зменшили ризик передчасних пологів.
Пренатальна добавка DHA збільшила вагу при народженні серед здорових доношених немовлят, але не зменшила ризик низької ваги при народженні.
Допологовий прийом DHA не підвищував ризик гестаційної гіпертензії або прееклампсії серед жінок з високим ризиком.
Добавки DHA не вплинули на моделі росту немовляти після пологів (вага, зріст або окружність голови).
Допологовий прийом DHA не вплинув на гостроту зору.
Для доношених немовлят дані про ефективність додавання дитячих сумішей з омега-3 були суперечливими, в залежності від того, коли і як оцінювалася гострота зору та в залежності від типу омега-3.
Добавки Омега-3 не мали стійкого впливу на неврологічний розвиток.
Добавки омега-3 або збагачені дитячі суміші не вплинуло на когнітивний розвиток доношених немовлят.
Добавки омега-3 не вплинули на розвиток розладу спектру аутизму, синдрому дефіциту уваги з гіперактивністю, атопічного дерматиту, алергії чи респіраторних розладів.
Прийом добавок DHA або EPA для матерів не впливали на ризик перинатальної депресії.
Автори не можуть виключити можливість того, що харчові добавки можуть допомогти людям із високим ризиком поганих результатів або людям із низьким рівнем DHA на початку дослідження:
“Кілька досліджень стратифікували результати відповідно до груп ризику, тому зазвичай було неможливо оцінити, чи залежить ефективність втручання з омега-3 від рівня ризику. Крім того, жодне рандомізоване контрольоване дослідження не стратифікувало результати за початковим рівнем жирних кислот омега-3, тому неможливо оцінити, чи може адекватність рівня жирних кислот омега-3 пояснити відмінності в результатах у дослідженнях (або відсутність результатів).”
В огляді Кокрейнівської бази даних [Middleton, 2018] виявили кілька статистично значущих впливів добавок омега-3, за винятком зниження ризику передчасних пологів і низької ваги при народженні. Статистично незначущі тенденції полягали в тому, що прийом добавок знижував ризик перинатальної смерті немовлят і госпіталізації новонароджених, а також знижувався ризик народження дітей з великою вагою для даного терміну вагітності. Ми обговоримо передчасні пологи (< 34 тижнів) детальніше, адже ці дослідження найперспективніші.
Довголанцюгові омега-3 і передчасні пологи
Кокрейнівський звіт виявив менший ризик передчасних пологів (Middleton, 2018). У звіті було включено принаймні одне дослідження, де використовувалася ALA, а не EPA або DHA [Mardones, 2008]; Я перерахував цифри після видалення цього дослідження та все одно виявив статистично значущий вплив (RR: 0,89, 95% CI: 0,80-0,99; Кількість потребуючих лікування: 66, 95% CI: 34-688; визначено за допомогою онлайн-калькулятора).
Ми зосередимося на висновках Кокрейна щодо передчасних пологів (< 34 тижнів), оскільки вони були сильнішими (2,7% проти 4,6%; RR: 0,58, 95% CI: 0,44-0,77; 9 рандомізованих контрольованих досліджень, 5204 учасниці), і наслідки потенційно шкідливіші.
Існує три причини, чому ваш Кокрейнівський звіт виявив більшу користь DHA при передчасних пологах, ніж звіт AHRQ:
Дані про те, що омега-3 знижують ризик передчасних пологів <34 тижнів переконливіші, ніж дані про зниження ризику передчасних пологів <37 тижнів, але звіт AHRQ проаналізував лише останні.
Кокрейнівський аналіз включав одне дослідження, [Mardones, 2008], де використовували ALA, а не DHA, та мали сильні висновки щодо зниження ризику ранніх передчасних пологів (RR: 0,19, 95% CI: 0,04-0,88), тоді як аналіз AHRQ не включав дослідження з використанням ALA.
У звіті AHRQ аналіз розділено на дослідження лише DHA (OR: 0,87, 95% CI: 0,66-1,15) і дослідження DHA + EPA (OR: 0,86, 95% CI: 0,65-1,15); поділ результатів на дві групи, ймовірно, послабив статистичну значущість.
Кокрейнівський звіт також включав три дослідження жінок з діабетом [Horvaticek, 2017] [Min, 2014] [Min, 2016], дослідження жінок з передчасними пологами в анамнезі [Bulstra-Ramakers, 1994], а також жінок із високим ризиком ускладнень вагітності [Olsen, 2000].
Я зібрав дослідження, використані в Кокрейнівському звіті, в електронну таблицю, Передчасні пологи. Після вилучення цих п’яти досліджень і дослідження з використанням ALA переваги DHA у запобіганні передчасним пологам < 34 тижнів залишалися (RR: 0,49, 95% CI: 0,24-0,71); Кількість потребуючих лікування: 60 (95% CI: 38-150). Я також розрахував статистичні дані для двох досліджень, які включали лише очевидно здорових учасниць і для яких тривалість вагітності була одним із основних результатів: RR: 0,24, 95% CI: 0,09-0,67; Кількість потребуючих лікування: 25, 95% CI: 15-72 [Carlson, 2013] [Harris, 2015].
На основі цих досліджень виявилося, що добавки DHA можуть допомогти запобігти передчасним пологам до 34 тижнів. Чи може ALA також запобігти їм?
Споживання ALA та передчасні пологи
[Mardones et al. (2008, Chile)] надавали малозабезпеченим вагітним жінкам сухе молоко, збагачене мікроелементами. Жінки в групі лікування також отримували ALA і LA. Використовуючи аналіз наміру лікування (аналіз, використаний у звіті Кокрейна), у групі лікування був нижчий ризик пологів до 34 тижнів (RR: 0,19, 95% CI: 0,04-0,88; Необхідна кількість для лікування (NNT): 59, 95% CI: 32-334). Однак якщо взяти аналіз під час лікування (жінок, які ретельніше дотримувалися протоколу), виявлення ALA є слабшим через меншу кількість передчасних пологів у групі плацебо (RR: 0,23, 95% CI: 0,05-1,07; Необхідна кількість для лікування (NNT): 54, 95 % CI: 28-1,117). Також вітамін B6 може бути фактором, оскільки група плацебо отримувала середнє значення рекомендованої норми (1,64 ± 0,66 мг), тоді як у групі лікування споживали на 30% більше (2,14 ± 1,21), що вище рекомендованої норми 1,9 мг для вітаміну B6 під час вагітності.
[Knudsen et al. (Denmark, 2006)] провели рандомізоване контрольоване дослідження добавок риб’ячого жиру або лляної олії серед понад 3000 вагітних жінок з низьким споживанням риби. Групи лікування складалися з щоденних добавок 100 мг EPA + DHA, 300 мг EPA + DHA, 700 мг EPA + DHA, 1400 мг EPA + DHA, 2800 мг EPA + DHA та 2600 мг ALA. Прийом добавки починався в середньому після 22 тижня вагітності і тривав до пологів. Не було виявлено жодних відмінностей у тривалості вагітності між групами, які приймали риб’ячий жир або лляну олію, порівняно з контрольною групою, яка не отримувала жодного втручання. Коли результати були обмежені жінками зі звичайним споживанням < 150 мг EPA + DHA на день, не було жодних ознак того, що добавки омега-3 збільшували тривалість вагітності на основі аналізу. Тривалість вагітності в контрольній групі жінок, які споживали менше 150 мг EPA + DHA на день, становила 40 тижнів, що свідчить про те, що ця популяція не піддається ризику передчасних пологів, незважаючи на низьке споживання довголанцюгових омега-3.
[de Groot et al. (2004)] провели подвійне сліпе, рандомізоване, контрольоване дослідження втручання з 14-го тижня вагітності до пологів. Початкове щоденне споживання ALA (на 14-му тижні вагітності) становило 1,3 г. Група лікування отримувала 2,8 г ALA + 9,0 г LA щодня порівняно з лише 10,9 г/день LA для контрольної групи. Споживання ALA контрольною групою вимірювали знову на 36-му тижні, воно становило 1,0 г/день. Середня тривалість вагітності в групі лікування була на 4,5 дня довшою, ніж у контрольній групі, що не було статистично значущим (P = 0,091). Частота передчасних пологів не вимірювалася.
Потрібні додаткові дослідження, щоб визначити, чи є дотримання рекомендованої норми ALA або збільшення споживання ALA так само ефективним, як DHA, для запобігання передчасним пологам.
Терміни втручання при ранніх (< 34 тижнів) передчасних пологах
У деяких дослідженнях застосування добавок DHA та передчасних пологів втручання розпочалося на досить пізніх термінах вагітності. Наша електронна таблиця Передчасні пологи перелічує терміни втручань без чіткої закономірності між часом і позитивним результатом.
Із трьох досліджень із використанням ALA в одному втручання було розпочато через 11 тижнів і було виявлено статистично значущий результат [Mardones, 2008], друге почалося на 14-му тижні та виявило незначну тенденцію [de Groot, 2004], а третє почалося на 22-му тижні без позитивного впливу [Knudsen, 2006]. Ці результати можуть бути випадковими.
Офіційні рекомендації
Станом на листопад 2022 року референтні норми Сполучених Штатів та Канади не рекомендують окремі добавки DHA під час вагітності або годування груддю.
Є й інші організації, які рекомендують DHA під час вагітності та годування груддю. Тут я детально розглядаю докази, використані Міжнародним товариством з вивчення жирних кислот і ліпідів (Society for the Study of Fatty Acids and Lipids, ISSFAL), а також включаю рекомендації Американської академії педіатрії (American Academy of Pediatrics).
Рекомендації ISSFAL щодо омега-3 під час вагітності та годування груддю
У 2007 році багато організацій, зокрема Міжнародне товариство з вивчення жирних кислот і ліпідів (ISSFAL), опублікували консенсусну заяву, яка рекомендує споживання DHA в середньому принаймні 200 мг на день під час вагітності та годування груддю. Вони використовували два напрями аргументів. Перший полягає в тому, що перетворення ALA в DHA обмежене:
“Фракційне перетворення a-ліноленової кислоти в n-3 LC-PUFA може бути більшим у жінок, ніж у чоловіків, що може сприяти задоволенню потреб у DHA плода та новонародженого, що перебуває на грудному вигодовуванні, але більшість доказів вказує на те, що загальний внесок a-ліноленової кислоти до створення в організмі DHA обмежений; отже, нормальне споживання попередньо сформованих n-3 LC-PUFA, і зокрема DHA, є важливим для підтримки оптимальної функції тканин (5-7)."
Для цього твердження посилалися на оглядову статтю [JT Brenna (2022)] який насправді є одним із авторів цієї консенсусної заяви. Однак я не знайшов цієї оглядової статті Бренни, яка б надала докази на користь цієї заяви. Навпаки, Бренна стверджує:
“Неможливість підвищити концентрацію 22:6n-3 [DHA] у крові за допомогою добавки 18:3n-3 [ALA] необов'язково означає, що концентрація 22:6n-3 не збільшується в тканинах. Перетворення та збереження 18:3n-3 може бути ефективним у розвитку нервової тканини та дуже активних тканин, таких як сітківка, яка активно повторно використовує 22:6n-3.”
Однак надійні вимірювання цих процесів неможливі без доступу до зразків тканин, а отже неможливі для більшості тканин у людей. Дослідження ефективності перетворення на тваринах мають обмежену цінність через фізіологічні відмінності, як зазначено нижче.
Джерело 6 була статтею [GC Burdge (2005)], де стверджується:
“Загалом [ALA] є обмеженим джерелом n-3 ПНЖК з довшим ланцюгом у людей. Таким чином, нормальне споживання попередньо сформованих n-3 ПНЖК з довгим ланцюгом, зокрема DHA, може бути важливим для підтримки оптимальної функції тканин.”
Однак, як зазначено в додатку до цієї статті, — Еволюційні аргументи на користь дієтичних потреб у DHA, — Бердж опублікував статтю у 2022 році, де стверджував, що ALA є нормальний джерелом для задоволення потреб немовлят у омега-3” [Burdge, 2022].
Джерело 7 — це огляд [SM Innis (2005)], що містить аналіз кількості DHA у мозку та стверджує, що недоношені немовлята не можуть виробляти достатню кількість DHA для забезпечення мозку такою кількістю. Але огляд, схоже, свідчить про те, що, як мінімум, ми не знаємо, чи можуть доношені діти отримати користь від добавки DHA.
Другий напрямок аргументів консенсусної заяви базується на клінічних випробуваннях добавок DHA під час вагітності та годування груддю, які, на думку авторів, показали сприятливий вплив на розвиток дитини. Вони цитують вісім клінічних випробувань, усі з яких включено до звіту Агентства з досліджень та якості охорони здоров’я (Agency for Healthcare Research and Quality) за 2016 рік, розглянутого вище [Newberry, 2016]. Ми детально обговорюємо це вище.
Рекомендації Американської академії педіатрії щодо DHA під час грудного вигодовування
У своєму технічному звіті — Грудне вигодовування та використання людського молока — Американська академія педіатрії (American Academy of Pediatrics) стверджує: «Харчування матері повинно включати в себе середньодобове споживання від 200 до 300 мг довголанцюгових поліненасичених жирних кислот омега-3 для отримання нормальної преформованої докозагексаєнової кислоти DHA в молоці матері та покращення рівня жирних кислот у немовляти [Meek and Noble, 2022]."
Американська академія педіатрії не надає обґрунтування своїх рекомендацій у цьому технічному звіті, але обґрунтування, яке вони надають у своєму виданні «Педіатричне харчування» за 2019 рік, не містить нічого важливого, що не було б розглянуто тут. Американська академія педіатрії не надає рекомендацій щодо вагітності.
Омега-3 і хронічні захворювання
Найбільше занепокоєння щодо низьких рівнів EPA та DHA у вегетаріанців викликано дослідженнями, які виявили зв’язок між низькими рівнями EPA та DHA в крові та підвищеним ризиком хронічних захворювань, як-от серцево-судинні захворювання, зниження когнітивних функцій і депресія.
Ці співвідношення загалом були послідовними, але слабкими. Були також певні зв’язки між рівнем омега-3 в крові та збільшенням деяких хронічних захворювань. У цьому розділі ми розглядаємо наявні докази.
Омега-3 і серцево-судинні захворювання
Дослідження омега-3 і серцево-судинних захворювань вивчили зв’язок із споживанням риби, рівнем омега-3 в крові та добавками омега-3.
Споживання риби та серцево-судинні захворювання
Станом на лютий 2021 року Американська кардіологічна асоціація (American Heart Association) все ще базувала свої рекомендації щодо омега-3 жирних кислот на своїх даних 2002 року — “Споживання риби, риб’ячий жир, омега-3 жирні кислоти та серцево-судинні захворювання” [Kris-Etherton, 2002], — де дорослим рекомендовано «вживати різноманітну (бажано жирну) рибу принаймні двічі на тиждень. Включіть олії та продукти, багаті альфа-ліноленовою кислотою (лляне насіння, рапсову та соєву олії; насіння льону та волоські горіхи).»
Деякі останні звіти надають такі дані:
Метааналіз шести когортних досліджень 2020 року не виявив кореляції між вживанням риби та зниженням ризику серцево-судинних захворювань або смертності [Zhong, 2020].
Кокрейнівський огляд 2020 року встановив, що недостатньо доказів для оцінки впливу вживання риби на здоров’я серцево-судинної системи [Abdelhamid, 2020].
Метааналіз 12 проспективних досліджень 2016 року виявив зниження ризику смертності при збільшенні споживання риби [Zhao, 2016].
Омега-3 і серцево-судинні захворювання
Кокрейнівський огляд 2020 року проаналізував 86 рандомізованих контрольованих досліджень тривалістю від 12 до 88 місяців із застосуванням капсул омега-3, збагаченої омега-3 їжі або дієтичних порад щодо вживання більше омега-3 [Abdelhamid, 2020]. Автори назвали це «найширшою систематичною оцінкою впливу жирів омега-3 на здоров’я серцево-судинної системи на сьогодні».
Цей огляд виявив незначний вплив збільшення споживання омега-3 на смертність від усіх причин або серцево-судинну смертність, серцево-судинні випадки, інсульт або аритмії. Збільшення споживання омега-3 показало тенденцію до зниження смертності від ішемічної хвороби серця (RR: 0,90, CI: 0,81-1,00) і спостерігалося зниження частоти випадків ішемічної хвороби серця (RR: 0,91, CI: 0,85-0,97).
Збільшення довголанцюгових омега-3 знижує тригліцериди на ~15% залежно від дози. Загалом автори заявили, що 334 людям потрібно буде збільшити споживання довголанцюгових омега-3, щоб запобігти ішемічній хворобі серця в однієї людини, і вони вважали, що цього недостатньо, щоб рекомендувати добавки.
На противагу цьому, метааналіз прийому добавок омега-3 у 2019 році виявив користь від прийому добавок омега-3 у комбінованих результатах 13 рандомізованих контрольованих досліджень із використанням приблизно від 800 до 1800 мг омега-3 жирних кислот на день [Hu et al.].
На початку в учасників був змішаний ризик серцево-судинних захворювань: у 40% був діабет, а 73% приймали ліки, що знижують рівень холестерину. В одному наборі результатів, який виключив дослідження REDUCE-IT, описане нижче, вони виявили зниження ризику серцевого нападу (RR: 0,92, CI: 0,86-0,99) і смерті від серцево-судинних захворювань (RR: 0,93, CI: 0,88-0,99).
Добавки омега-3 у цьому наборі результатів, можливо, перевищують рекомендації AHA щодо принаймні 2 порцій риби на тиждень, але це не є неправдоподібним. Про вміст омега-3 в рибі див. Омега-3 жирні кислоти: інформаційний бюлетень для медичних працівників.
Дослідження «Дослідження зменшення серцево-судинних подій при застосуванні етилового інтервенційного препарату ікосапент (REDUCE-IT)» (The Reduction of Cardiovascular Events with Icosapent Ethyl-Intervention Trial (REDUCE-IT)) було виключено з результатів Hu та ін., наведених вище, оскільки в ньому використовувалася набагато більша доза омега-3: 4000 мг/день очищеної форми EPA. Було виявлено помітно кращий успіх при серцевому нападі (RR: 0,69, CI: 0,58-0,81) і смерті від серцево-судинних захворювань (RR: 0,80, CI: 0,66-0,98).
Учасники дослідження також мали нижчий ризик інсульту (RR: 0,72, CI: 0,55-0,93), але відносний ризик їхньої смертності від усіх причин не був статистично значущим, хоч і нижчим (RR: 0,87, CI: 0,74-1,02), в порівнянні з групою плацебо [Bhatt, 2019]. Надзвичайно велика кількість EPA, що використовується в REDUCE-IT, є фармакологічною дозою і не має відношення до споживання омега-3 з їжею.
Інсульт і співвідношення омега-6 і омега-3
[Cupino et al. (2022)] проаналізували співвідношення споживання омега-6 і омега-3 і ризик інсульту серед когорти Adventist Health Study-2. Вони виявили статистично значущий зв’язок між співвідношенням омега-6 і омега-3 і підвищеним ризиком будь-якого типу смертельного інсульту (HR: 1,40, 95% CI: 1,16-1,69) для співвідношення 90-го процентиля (12:1) проти 10-го процентиля (6:1).
Омега-3 і когнітивні функції
У перехресному звіті Фремінгемського дослідження 2012 року (Framingham Study) було обстежено 1575 осіб (54% жінок) із середнім віком 67 років (Стандартне відхилення: 9 років) щодо рівня омега-3 в крові та численних когнітивних параметрів [Tan, 2012].
Дослідники порівняли жирні кислоти мембрани еритроцитів EPA+DHA у найнижчому квартилі (≤4,4%) з жирними кислотами у верхніх трьох квартилях (75-й процентиль становив 6,5%). Вони виявили, що в тих, хто перебуває в нижчому квартилі, об’єм головного мозку був значно нижчим (еквівалентний приблизно дворічному старінню мозку), але подібний об’єм гіперінтенсивності білої речовини, об’єм скроневого рогу та частота тихого інсульту. Низький рівень EPA+DHA в крові був пов’язаний із гіршою оцінкою за деякими тестами.
У межах дослідження когнітивного старіння Ініціативи жіночого здоров’я [Ammann et al. (2013, USA)] (Women’s Health Initiative Study of Cognitive Aging) провели перехресний аналіз 2302 жінок віком від 65 років і не виявили різниці в когнітивних функціях між жінками у верхній третині порівняно з жінками у нижній третині відсоткового розподілу EPA + DHA жирних кислот у еритроцитах. Проте для найнижчої третини середній показник EPA + DHA був 3,8%, що трохи вище, ніж у веганок, тому цей висновок необов’язково заспокоює нас щодо рівня омега-3 у веганів. Дослідження 2017 року Ammann та ін. (описано нижче), аналізувало значно більшу групою учасників протягом певного часу та дає краще розуміння того, чи важливі вищі відсотки EPA та DHA для запобігання когнітивним порушенням і деменції, особливо у літніх жінок.
[Zhang et al. (2016)] провели метааналіз 21 дослідження типу «випадок-контроль» і проспективних досліджень та виявили, що збільшення кількості риби на 1 порцію/тиждень було пов’язане зі зниженим ризиком деменції (RR: 0,95, CI 0,90-0,99) і хвороби Альцгеймера (RR: 0,93, CI: 0,90-0,95). Споживання DHA також було обернено пов’язане з ризиком деменції (RR: 0,86, CI: 0,76-0,96) і хвороби Альцгеймера (RR: 0,63, CI: 0,51-0,76).
Однак рівні омега-3 жирних кислот у крові не були пов’язані зі зниженням ризику тих чи інших когнітивних захворювань. У листі до редактора Koch and Jensen зазначають, що в шести дослідженнях, присвячених зв’язку між споживанням риби та деменцією і хворобою Альцгеймера, одне дослідження було дворічним продовженням іншого дослідження з більш тривалим спостереженням.
[Koch and Jensen] стверджують що «Належне виключення звіту Kalmijn та ін. зробило б дані метааналізу споживання риби щодо ризику розвитку деменції статистично незначущими (RR: 0,96; 95% CI: 0,91, 1,01; відсутність гетерогенності) і змінив оцінку відносного ризику для хвороби Альцгеймера на 0,87 (95% CI: 0,77, 0,98) у метааналізі випадкових ефектів із досі значною гетерогенністю між дослідженнями».
[Zhang and Jiao] відповіли, що доцільно включити обидва звіти. Викликає подив те, що споживання омега-3, але не рівень в крові, буде пов’язано зі зниженим ризиком деменції, якщо є справжній ефект, хоча це може дати підставу припустити, що рівні EPA та DHA в крові не є точним відображенням рівня омега-3.
[Amman et al. (2017, USA)] провели найбільше проспективне дослідження для оцінки ризику деменції з різними статусом омега-3 жирних кислот. Дослідження було частиною дослідження пам’яті Ініціативи жіночого здоров’я (Women’s Health Initiative Memory Study), яке вивчало вплив гормонів естрогену та прогестину на пам’ять жінок віком ≥65 років. Незважаючи на те, що гормональна частина дослідження була завершена на ранній стадії, дослідники продовжували спостерігати за 6706 жінками в середньому протягом 9,8 років, щоб з’ясувати, чи пов’язані базові рівні EPA та DHA з діагнозом ймовірної деменції або легкого когнітивного порушення.
У дослідженні порівнювали ризик деменції і когнітивних порушень серед тих, у кого EPA/DHA у межах одного стандартного відхилення вище середнього (5,3-6,8% EPA+DHA) з тими, хто знаходиться в межах одного стандартного відхилення нижче середнього (3,8-5,3% EPA+DHA). В одній зі своїх моделей дослідники виявили статистично значуще зниження ризику деменції (HR: 0,91, CI: 0,83-0,99), але більшість моделей не виявили суттєвого зв’язку, включно з тією, яка коригувала генотип APOE, пов’язаний із хворобою Альцгеймера (HR: 0,92, CI: 0,83-1,01).
Дослідники підрахували, що підвищений ризик хвороби Паркінсона означає зниження ризику захворювання на хвороби серця на 2% (12% проти 14%) протягом 15-річного періоду. Не було виявлено суттєвого зв’язку між EPA+DHA та когнітивними порушеннями. Дослідження EPA та DHA окремо не дало значущих результатів.
Таким чином, дослідження омега-3 жирних кислот, проведені на популяціях всеїдних, постійно виявляють певний зв’язок із кращими когнітивними здібностями, хоча цей зв’язок, як правило, слабкий. Те, що споживання їжі сильніше пов’язане з кращими когнітивними функціями, ніж рівень кислот у крові, викликає питання про те, чи саме омега-3 відповідають за сприятливий зв’язок, а не інші змінні, пов’язані зі споживанням омега-3.
Омега-3 і депресія
Наш інтерес до омега-3 і депресії здебільшого пов’язаний із тим, чи вегетаріанці піддаються підвищеному ризику депресії через низькі рівні EPA або DHA.
Ризик депресії
[Deane et al. (2019)] провели метааналіз і систематичний огляд 32 рандомізованих контрольованих досліджень і не виявили впливу збільшення EPA і DHA на ризик симптомів депресії (RR: 1,01, CI: 0,92-1,10). Дослідження мали середню тривалість 12 місяців із середньою дозою 0,95 г на день (від 0,4 до 3,4 г на день). Одне дослідження розглядало омега-3 і тривожність і не виявило практично ніякого ефекту. Дослідники рекомендують не приймати добавки омега-3 для зниження ризику депресії та тривоги.
Лікування депресії
Питання про те, чи можна EPA або DHA використовувати для лікування людей із депресією, лише незначною мірою пов’язане з рівнем омега-3 у вегетаріанців, але саме на цьому зосереджена більшість досліджень, тому ми розглядаємо це тут.
Ранні дослідження щодо лікування симптомів депресії за допомогою добавок EPA та DHA були неоднозначними. В огляді 2006 року [Sontrop and Campbell] виявили, що добавки полегшують депресію, але не було зрозуміло, чи ефективні вони для пацієнтів із депресією загалом чи лише для тих, у кого аномально низькі концентрації EPA та DHA.
В іншому огляді 2006 року [Appleton et al.] виявили «невелику підтримку» тези щодо позитивного впливу EHA+DHA на основі невеликої кількості випробувань зі значними варіаціями. У метааналізі 2007 року [Lin and Sue] виявили позитивний ефект добавок, але публікація мала значне упередження публікації. У метааналізі 2009 року [Martins] виявив докази того, що EPA є ефективнішою за DHA.
[Grosso et al. (2014)] провели метааналіз 11 випробувань пацієнтів із визначеним за DSM діагнозом великого депресивного розладу і 8 випробувань пацієнтів із депресивною симптоматикою, але без діагнозу. Дослідники виявили, що добавки мають сприятливий ефект для пацієнтів із діагнозом, а також для тих, хто має біполярний розлад. Вони вважали EPA більш ефективним, при цьому у багатьох дослідженнях використовували фармакологічні дози. [Hallahan, et al. (2016)] дійшли до подібних результатів у своєму метааналізі.
У своєму метааналізі [Luo et al. (2020)] виявили користь від високих доз (≥2 г/день), але не низьких доз (<2 г/день), добавок EPA/DHA на ранньому періоді терапії.
Омега-3 і підвищений ризик захворювань
Деякі дослідження пов’язують високе споживання омега-3 з підвищеним ризиком певних захворювань.
Рак простати
Метааналіз рандомізованих контрольованих досліджень [Hanson, 2020] вимірював вплив на ризик діагностики раку простати більшого споживання довголанцюгових омега-3 (7 досліджень, RR: 1,10, 95% CI: 0,97-1,24, Необхідна кількість для ризику, NNTH: 334) і більшого споживання ALA (2 дослідження, RR: 1,30, 95% CI: 0,72–2,32, Необхідна кількість для ризику, NNTH: 334). Жоден результат не був статистично значущим і мав високу необхідну кількість для ризику (NNTH). Не було виявлено жодного впливу на загальну діагностику раку або смерть. Автори надали діаграму, яка показує, що переваги більшого споживання омега-3 на серцево-судинну систему переважають потенційну шкоду.
Метааналіз [Carleton, 2013] досліджень типу «випадок-контроль» і проспективних досліджень не виявив зв’язку між прийомом ALA і раком простати (RR: 1,08, 95% CI: 0,90-1,29). Видалення одного дослідження під час аналізу чутливості призвело до слабкого, незначного захисного ефекту для ALA (RR: 0,91, 95% CI: 0,83-0,99, p=0,02).
Систематичний огляд і метааналіз [Simon, 2009] концентрації ALA в крові або тканинах і раку передміхурової залози не виявили зв’язку після поправки на упередження публікації (RR: 0,96, 95% CI: 0,79-1,17).
Метааналіз 2010 року показав, що суб’єкти, які споживали більше 1,5 г ALA на день, мали значно менший ризик раку простати (0,95, 0,91-0,99) порівняно з тими, хто споживав менше [Carayol, 2010].
У статті Гарвардської школи громадської охорони здоров’я 2018 року було припущено, що минулий зв’язок між ALA і раком передміхурової залози міг бути пов’язаний з транс-ALA, яка була значною мірою вилучена з ланцюжка постачання продуктів харчування (законодавчо і не тільки - прим.ред.) [Wu, 2018].
Дослідження типу “випадок-контроль” із випробування SELECT [Brasky, 2013] виявило зв’язок між високими рівнями фосфоліпідів DHA та раком простати. Цей висновок замінений висновками Hanson et al. (2020), описаними вище, але дискусія щодо цього висновку з 2013 року можна знайти в публікації блогу JackNorrisRD.com: Добавки DHA та рак простати. [[blog]]
Зір
Аналіз дослідження здоров’я медсестер (Nurses Health Study) 2001 року виявив майже статистично значуще збільшення вікової макулодистрофії у тих, хто споживає найбільше ALA [Cho, 2001, USA].
На противагу цьому, дослідження 2013 року показало, що вищі рівні ALA в крові пов’язані з меншим ризиком пізньої вікової макулодистрофії [Merle, 2013, France]. Подальший аналіз Дослідження медсестер у 2017 році показав, що високе споживання ALA було пов’язане з підвищеним ризиком проміжної вікової макулодистрофії до 2002 року, але не пізніше, коли в крові учасників було виявлено менше транс-жирів [Wu, 2017, USA].
Аналіз дослідження здоров’я медсестер 2005 року показав, що найвище споживання ALA і LA було пов’язане зі збільшенням помутніння кришталика, що може призвести до катаракти [Lu, 2005, USA]. Для ALA співвідношення ризику становило 2.2 (1.2, 4.5) для приблизно 1,26 г порівняно з 0,86 г на день. Аналіз тієї ж групи у 2007 році виявив, що найвища категорія споживання ALA (приблизно 1,26 г на день) була пов’язана зі збільшенням ядерної щільності кришталика ока на 16% порівняно з найнижчою категорією (приблизно 0,84 г на день) протягом п’яти років. Станом на 2018 рік, схоже, жодних подальших аналізів щодо ALA та катаракти в рамках того ж дослідження не проводилося [Lu, 2007, USA].
Без більш детальних досліджень ми не вважаємо, що занепокоєння щодо зору є причиною уникати рослинних джерел ALA через наступне: невеликі відмінності в споживанні ALA в цих дослідженнях; той факт, що велика кількість ALA у всеїдних раціонах надходить з продуктів тваринного походження; той факт, що трансжири більше не додаються до харчових продуктів; а також через багато неузгодженостей досліджуваних зв’язків між різними жирними кислотами та різними станами здоров’я.
Додаток A: Біомаркери рівнів DHA
Основною причиною, чому дослідники покладаються на відсотковий вміст DHA у плазмі та/або еритроцитах, є зручність: це найбільш доступні та прості вимірювання. Дослідження постійно виявляють зворотні зв’язки, хоч і слабкі, між відсотками вмісту DHA у крові та захворюваністю, що сприяє їхньому використанню.
У своєму огляді біомаркерів рівня DHA [Kuratko and Salem (2009)] стверджують, що відсоток жирних кислот у вигляді DHA у плазмі або еритроцитах є в принципі адекватним маркером загального рівня DHA. Однак вони також підкреслюють багато застережень, які ми обговорюємо вище у розділі Перетворення ALA в EPA і DHA.
Куратко і Салем цитують одну статтю, яку варто тут обговорити. У жахливому експерименті, [Sarkadi-Nagy et al. (2004)] досліджували немовлят павіанів, щоб виміряти різні жирні кислоти у їхній крові та тканинах. У віці 14 днів немовлятам дали дозу ALA, мічену вуглецем. Ще через 14 днів їх було вбито, і дослідники виміряли кореляції між DHA, міченою вуглецем, у плазмі та еритроцитах із DHA, міченою вуглецем, у мозку, сітківці та печінці. R-коефіцієнти наведені в таблиці нижче.
Куратко та Салем узагальнюють результати Sarkadi-Nagy та ін.: «Рівні в еритроцитах і плазмі корелюють із кінцевим вмістом DHA в мозку, сітківці та печінці». Але ці кореляції не були виявлені між загальним відсотком жирних кислот типу DHA; радше це був відсоток жирних кислот у вигляді DHA, які були перетворені з ALA протягом періоду дослідження.
На противагу цьому, у своїй таблиці 3 Sarkadi-Nagy та ін. перераховують загальну кількість різних жирних кислот у плазмі, червоних кров’яних тільцях і тканинах, і хоча були деякі подібності, було також багато відмінностей.
Sarkadi-Nagy та ін. пишуть: «Загальновідомо, що концентрація [жирної кислоти] в тканинах і плазмі залежить від харчування. Покращення функцій організма не можна припустити, його необхідно продемонструвати (43). Крім того, великі варіації в регуляції індивідуальних концентрацій [жирних кислот] від тканини до тканини ускладнюють екстраполяцію з джерел вимірювання, доступних у людини, насамперед із плазми та еритроцитів». Інакше кажучи, для підкріплення своєї точки зору, що рівень DHA в крові є адекватним маркером рівня омега-3, Kuratko і Salem покладаються на статтю Sarkadi-Nagy та ін., які не погоджуються з тим, що показник стану тканини можна екстраполювати з відсоткового вмісту крові.
Куратко та Салем також цитують дослідження на мавпах-резусах, а потім підсумовують, заявляючи: «Хоча статистична кореляція не була повідомлена, очевидно, що існує позитивний зв’язок між рівнями DHA в еритроцитах і рівнями в тканинах, включаючи кору головного мозку та сітківку ока [68,69].” Їхнє джерело №68, [Pawlosky et al. (1997)], — дослідження, де не вимірювався рівень жирних кислот в еритроцитах. Їхнє джерело №69, — [Pawlosky et al. (2001(a))], — дослідження, де використовували вуглецевий індикатор для вимірювання перетворення ALA в EPA і DHA в крові людини, але не в тканинах.
Стаття Куратко і Салема також містить посилання №58, на дослідження [Pawlosky et al. (2001(b))], де йдеться про дослідження з використанням макак-резусів, але документ був недоступний, а анотація не вказує на те, що дослідження підтвердить їхню заяву.
На момент написання статті Куратко та Салем були співробітниками Martek Biosciences, — компанія, ймовірно, могла б отримати вигоду від зручного біомаркера рівня DHA, який би дав підставу переоцінювати потребу в добавках DHA.
Імовірно, є багато інших досліджень, не згаданих у цій статті, які проводили різні порівняння між відсотками довголанцюгових омега-3 жирних кислот у крові та тканинах. Кореляції дійсно існують у деяких популяціях, але вони доволі нечіткі та не можуть бути використані для того, щоб зробити будь-які певні висновки щодо рівня омега-3 у зовні здорових людей.
Додаток B: Еволюційні аргументи на користь дієтичних потреб у DHA
Поживна речовина є важливою, якщо вона повинна надходити в раціон для оптимального здоров’я. Поживна речовина є умовно необхідною, якщо вона потрібна в раціоні лише за неоптимальних умов.
Існує еволюційний аргумент про те, що DHA є важливою поживною речовиною, який звучить так:
“Протягом тривалого періоду нашої еволюції люди жили поблизу великих водойм, які забезпечували рясні джерела харчової DHA через рибу. Ця велика кількість DHA дозволила людському мозку збільшитися в розмірах і збільшити інтелект. Як наслідок, люди все ще залежать від джерела харчової DHA для оптимального стану мозку.”
Жири з коротким ланцюгом омега-3 і омега-6 конкурують за ті самі ферменти, щоб перетворюватись в довголанцюгові відповідники. Через це також існує еволюційний аргумент, що DHA є умовно необхідною поживною речовиною:
“У сучасних дієтах люди споживають таку велику кількість омега-6 жирів, що здатність організму виробляти достатню кількість DHA, щоб конкурувати з омега-6, порушується. За неоптимальних умов високого споживання омега-6 харчова DHA стає важливою.”
Я зосереджуся насамперед на першому еволюційному аргументі — чи потрібне людям харчове джерело DHA через еволюційну залежність від вживання риби. Однак дослідження, які я розгляну, іноді змішують ці два аргументи, тому я хотів описати їх обидва на початку.
Є чотири етапи життя, коли DHA може бути незамінною або умовно необхідною:
Під час внутрішньоутробного розвитку плід принаймні частково залежить від отримання DHA від матері.
Немовлята можуть бути залежними від харчового джерела DHA з грудного молока матері або харчової суміші.
Під час вагітності або годування груддю без харчового джерела DHA мати може бути не в змозі перетворити достатню кількість ALA в DHA, щоб забезпечити себе та потреби своєї дитини.
У дорослому віці може знадобитися харчове джерело DHA, щоб запобігти погіршенню когнітивних функцій.
Питання про те, чи потрібне немовлятам харчове джерело DHA для оптимального розвитку мозку, не має відношення до аргументу, що люди еволюціонували залежно від споживання риби, оскільки немовлята можуть отримувати DHA з грудного молока, тому я не витрачаю багато часу на розгляд цього питання.
Я також не розглядаю аргументи щодо джерел їжі несучасної людини, тому що навіть якщо стародавня людина їла достатню кількість риби, це не повинно означати, що сучасні люди мають харчові потреби в DHA.
Натомість я переглядаю докази того, що я вважаю найбільш переконливими аргументами на користь важливості харчової DHA. Деякі з цих аргументів є екологічними, наприклад, твердження про те, що розмір людського мозку та інтелект зменшилися, а неврологічні проблеми та психічні захворювання зросли через відмову від харчування з високим вмістом морепродуктів. Я також розглядаю конкретні фізіологічні твердження щодо метаболізму омега-3 на основі клінічних досліджень. У більшості цих досліджень використовувалися тварини.
Нижче я розглядаю три опубліковані статті, які стверджують, що люди еволюціонували на дієті, яка включала рибу, тобто таким чином і постійне харчове джерело DHA, яке збільшило розмір нашого мозку та інтелект. Вони означають, що ми все ще залежимо від харчової DHA для оптимального розвитку та підтримки мозку. Я також переглядаю дві статті, у яких стверджується, що немає потреби в DHA після віку немовлят.
Кроуфорд, 2006, Кроуфорд та ін., 2022
Майкл А. Кроуфорд є дослідником з Інституту хімії мозку та харчування людини у Великобританії. Він публікував наукові статті, інколи разом із співавторами, стверджуючи, що в сучасному світі нехтують поживними речовинами омега-3, а харчові джерела DHA є важливими для еволюції людського мозку і все ще важливими для розвитку мозку немовлят.
Я розповім про те, що вважаю найпереконливішими аргументами в його статтях: [Докозагексаєнова кислота в нейронних сигнальних системах (2006)] і [Нейророзвиток, харчування та генетика (2022)].
Стаття Кроуфорда 2006 року, здається, є відповіддю на статтю [Джона Ленґдона 2006] року, у якій стверджується, що немає еволюційних вимог для DHA після віку немовлят (я розглядаю її далі). Кроуфорд каже, що «[Ленґдон] нехтує основним принципом дарвінівської еволюції. Добре задокументована більша ефективність попередньо сформованої докозагексаєнової кислоти для постачання в тканини мозку під час розвитку мала б дати явну перевагу у виживанні порівняно з тими, хто не мав її».
Але, незважаючи на численні аргументи та цитати, Кроуфорд наводить лише припущення про те, що для правильного розвитку людського мозку необхідне харчове джерело DHA, крім грудного молока. Натомість він наводить докази того, що омега-3, які можуть бути у формі ALA, необхідні.
Наприклад, [Crawford (2006)] пише, що «DHA в раціоні швидко та вибірково вбудовується в мембрани клітин головного мозку та концентрується в синаптичних сигнальних місцях [Suzuki et al., 1997].» У цьому дослідженні Suzuki та ін. мишей-самців позбавляли омега-3 протягом 11 днів, а потім поміщали в групу дієти на 6 або 30 днів. Існувало багато груп мишей, але я обмежу цей підсумок дієтичними групами без прийому омега-3, з прийомом ALA і з прийомом DHA. У таблиці нижче показано рівні DHA серед різних груп мишей наприкінці кожного випробування.
Рівні в плазмі крові істотно відрізняються, тоді як рівні в мозку однакові. Фізіологічне значення відмінностей у відсотковому вмісті DHA у мозку між групами, які отримували ALA та DHA, не було визначено.
Можливо, це дослідження дає впевненість, що, принаймні для мишей, ALA як єдине дієтичне джерело омега-3 може бути достатнім. Але оскільки миші в дикій природі навряд чи еволюціонували зі значним джерелом харчової DHA, ці результати необов’язково можна застосувати до людей.
Кроуфорд (2006) пише:
“Дослідження дефіциту у гризунів (Sinclair and Crawford, 1973), приматів (Fiennes та ін., 1973, Neuringer та ін., 1976), а також зорові та когнітивні дослідження немовлят (Birch та ін., 2000) показали, що DHA є важливою для розвитку і функціонування мозку.”
[Sinclair and Crawford (1973)] не ізолювали DHA жодним чином, щоб виправдати це твердження. [Fiennes et al. (1973)] досліджували дефіцит омега-3, а не дефіцит DHA. [Neuringer et al. (1986)] вивчали дієти з низьким вмістом ALA. [Birch et al. (2000)] показали, що немовлята, які не були на грудному вигодовуванні, але мали DHA у дитячій суміші, показали кращі результати в деяких когнітивних і моторних тестах, ніж немовлята без DHA у суміші.
На епідеміологічному рівні Кроуфорд стверджує, що відмова від харчування з морепродуктами в основі спричинила дефіцит важливих поживних речовин, особливо DHA та йоду, що призвело до глобального зростання психічних розладів, а також зменшення інтелекту та розміру мозку. Я зупинюся на цих моментах, але, оскільки ці теми дуже об’ємні, я роблю лише побіжний огляд.
Психічне здоров'я та розлади мозку
Кроуфорд (2006) пише:
“Зростання психічних розладів і розладів мозку, витрати на які витісняють інші витрати в європейському списку тягарів проблем здоров’я, порушує цікаві питання щодо їхнього зв’язку зі зменшенням доступності та споживання харчових продуктів з походженням з морської та прісної фауни.
У 1972 році, спираючись на зміни у наукових знаннях про харчування та ліпіди, ми передбачили, що розлади мозку зростуть, і це сталося. Розлади головного мозку зараз спричиняють найвищу вартість витрат на лікування проблем зі здоров’ям в ЄС (386 мільярдів євро), обігнавши серцево-судинні захворювання, рак і ожиріння з великим відривом. Це не дивно. Мозок спочатку розвинувся в морі і досі використовує морські жирні кислоти; втрата морської гілки харчового ланцюга неодмінно матиме наслідки.”
У 2022 році Кроуфорд та ін. продовжують наголошувати на цьому аргументі, кажучи: «У 2019 році, до пандемії, кожен п’ятий дорослий у США жив із психічними захворюваннями [Національний інститут здоров’я]; 197,3 мільйонів в Індії, які страждають на психічні розлади в 2017 році, є числом того ж порядку, двозначним відсотком від усього населення [GBD India]».
Чи правий Кроуфорд у тому, що захворювання мозку та психічні захворювання зростають?
Згідно зі статтею, [Глобальний, регіональний та національний тягар витрат на лікування неврологічних розладів, 1990–2016 рр.], абсолютна кількість неврологічних розладів зростає через старіння населення, але після поправки на вік та інші змінні показники фактично зменшуються. Для цього аналізу вони включили широкий спектр захворювань, деякі з яких навряд чи пов’язані з дефіцитом DHA. Ось список деяких конкретних захворювань і відсоток збільшення (+) або зменшення (-) захворюваності з поправкою на вік між 1990 і 2016 роками: інсульт (-8%), хвороба Альцгеймера та інші деменції (+2%), хвороба Паркінсона (+22%), ідіопатична епілепсія (+6%), розсіяний склероз (+10%) та мігрень (-2%).
Стосовно психічних захворювань Кроуфорд та ін. (2022) цитують веб-сторінку Національного інституту здоров’я: Психічні хвороби. Хоча на сторінці не оцінюється, чи зростає кількість психічних захворювань, дослідники стверджують, що будь-які психічні захворювання вражають великий відсоток дорослих у США (21% станом на 2020 рік). Це може бути психічний, поведінковий або емоційний розлад і він може варіюватися за порушенням: від відсутності до легкого, помірного або важкого.
Що стосується важких психічних захворювань, поширеність становила 5,6% усіх дорослих у США, при цьому вона була вищою серед дорослих віком 18-25 років (9,7%), ніж дорослих віком 26-49 років (6,9%) і віком 50+ (3,4%). Згідно з даними Опитування підлітків до Національного дослідження коморбідності (National Comorbidity Survey Adolescent Supplement), у 49,5% підлітків був якийсь розлад; 22,2% із них мали важкі порушення.
Стосовно психічних захворювань в Індії, Кроуфорд та ін. (2022) цитують статтю [Тягар витрат на лікування психічних розладів у штатах Індії: дослідження глобального тягаря хвороб, 1990-2017 рр.] Там виявлено, що внесок психічних розладів у сумарну кількість років життя з поправкою на інвалідність (disability-adjusted life-years, DALY) в Індії зріс з 2,5% у 1990 році до 4,7% у 2017 році. У 2017 році депресивні розлади складали найбільшу відносну частку (33,8%) в загальному показнику DALY, далі йдуть тривожні розлади (19,0%), ідіопатична інтелектуальна недостатність (10,8%), шизофренія (9,8%), біполярний розлад (6,9%), розлади поведінки (5,9%), розлади аутистичного спектру (3,2%), розлади харчування ( 2,2%) та синдром дефіциту уваги з гіперактивністю (0,3%). Деменція не згадувалася у цьому звіті.
Ці показники психічних захворювань дійсно здаються досить високими, але деякі припускають, що це пов’язано з більшою кількістю звітів. Стаття в The Guardian — Психічні захворювання: чи справді існує глобальна епідемія? (3 червня 2019 р.) — повідомляє, що за попередні 20 років дві змінні впливали на рівень психічних захворювань: визнання та дестигматизація. Це призвело до того, що більше людей звертаються за допомогою та повідомляють про психічний розлад. Гарві Вайтфорд, професор психічного здоров’я населення з Університету Квінсленда, цитує: «Усе моделювання, яке ми проводили в країнах з високим рівнем доходу, де є дані опитувань, які відстежували з часом, показує, що поширеність не змінилася, — вона на тому ж рівні.
Ідея про те, що розлади мозку та психічні захворювання зростають через нестачу дієтичної DHA, є цікавою гіпотезою, яку, втім, важко оцінити.
Інтелект
Кроуфорд та ін. (2022) стверджують, що світовий середній коефіцієнт інтелекту (IQ) досяг свого піку в 1975 році народження, а потім постійно знижувався до 1990 року народження. Хоча графік 1 у їхній статті демонструє постійну тенденцію, різниця становить лише близько 2,5% від нормального IQ.
Норвегія є цікавим випадком щодо зниження IQ порівняно зі споживанням риби на душу населення. Стаття із Всесвітнього економічного форуму — IQ падає — і так було роками (2018) — наводить дані з Норвегії, де чоловіки, які проходили військову службу між 1970 і 2009 роками, проходили тести на IQ.
«[Аналіз] показав, що чоловіки, які народилися в 1962 році, мали вищі бали, ніж ті, хто народився в 1991 році. Ті, хто народився в 1991 році, набрали на п’ять балів нижче, ніж ті, хто народився в 1975 році, і на три бали нижче, ніж ті, хто народився в 1962 році. Результати протилежні тому, що відбувалося протягом більшої частини 20 століття, коли показники IQ зростали приблизно на 3% на рік».
Норвегія має одне з найвищих рівнів споживання риби на душу населення серед усіх країн. HelgiLibrary створила графік, використовуючи дані FAOSTAT: Споживання риби на душу населення в Норвегії, демонструючи збільшення з приблизно 41 кг у 1960 році до приблизно 53 кг у 2013 році. Збільшення споживання риби на душу населення в Норвегії протягом того часу, коли IQ знижувався, свідчить про те, що зниження IQ не було спричинене падінням споживання риби.
Норвегія була єдиною країною, для якої я знайшов достатньо доступні дані, щоб зробити це порівняння. Виходячи з цих даних з Норвегії, здається малоймовірним, що зниження інтелекту пов’язане з відходом від дієти, заснованої на морепродуктах.
Розмір мозку
Кроуфорд та ін. (2022) пишуть:
Доктор Марта Лар з Центру еволюційних досліджень людини Кембриджського університету Великобританії представила Королівському товариству у 2013 році свої висновки про те, що розмір мозку сучасної людини зменшувався з початку наземного землеробства та тваринництва 10 000 років тому.
Для цього твердження Кроуфорд та ін. процитувати коротку новинну статтю, Сільське господарство винне у тому, що наші розміри та розум зменшуються (авторка Дебора Браконьє, Phys.org, 2011).
Ця стаття закінчується словами:
“Однак сільське господарство не пояснює зменшення розміру мозку. Лар вважає, що це може бути результатом впливу більших потреб в енергії, необхідної для підтримки великих розмірів мозку… Однак це зменшення розміру мозку не означає, що сучасні люди менш розумні. Людський мозок еволюціонував, щоб працювати ефективніше та споживати менше енергії.”
У пов’язаній статті — Чи мізки зменшуються, щоб зробити нас розумнішими? (Жан-Луї Сантіні, Phys.org, 2011) — говориться:
“Але скорочення розміру не означає, що сучасні люди дурніші за своїх предків — радше вони просто розвинули інші, більш витончені форми інтелекту, — сказав Браян Хейр, доцент кафедри антропології в Університеті Дьюка.”
Стаття 2019 року від Discover — Людський мозок стає меншим з кам’яного віку (Бріджит Алекс) — стверджує, що найвірогідніше пояснення зменшення розміру людського мозку полягає у виживанні найдружніших:
“Ідея полягає в тому, що в суспільствах кам’яного віку в кооперативних, врівноважених індивідів було більше шансів вижити й розмножуватися, ніж у войовничих, агресивних. На ці про- чи антисоціальні нахили впливали гени, що регулюють гормони, що також впливало на фізичні риси, включаючи розмір тіла та мозку. З часом «виживання найдружніших» призвело до того, що люди мали в середньому меншу статуру та мізки. Тож хоча відбулося зменшення розміру черепа — і, можливо, інтелекту — людська співпраця посилилась, формуючи глибшу колективну мудрість.”
Я не вважаю ці новинні статті науково обґрунтованими, але вони свідчать про те, що відмова від дієти з морепродуктами не є загальноприйнятим поясненням зменшення розміру мозку і що це зменшення розміру мозку не є ознакою проблем здоров’я.
Генетика та співвідношення n6:n3
Кроуфорд та ін. (2022) висунули теорію про те, що традиційні вегетаріанські суспільства, такі як регіон Пуна в Індії, як правило, мають генетичні особливості перетворення жирних кислот, які призводять до низького перетворення ALA в DHA, коли споживання омега-6 є високим (наприклад, у сучасних дієтах), незалежно від того, скільки ALA додано до раціону. Якщо це правда, DHA буде умовно необхідною поживною речовиною в цих контекстах, але це відрізняється від твердження, що люди еволюційно мають дієтичні потреби в DHA через залежність від харчування морепродуктами та продуктами водної фауни.
Бредбері, 2011
У 2011 році доктор Джоан Бредбері зі Школи здоров’я та гуманітарних наук Університету Південного Хреста в Австралії опублікувала статтю — [Докозагексаєнова кислота (DHA): давня поживна речовина для сучасного людського мозку].
Бредбері стверджує, що сучасні люди пристосувалися до споживання попередньо сформованої DHA. Аргументи Бредбері ґрунтуються на ідеї, що ендогенний синтез DHA з ALA у людей є «набагато нижчим і обмеженішим, ніж передбачалося раніше». Бредбері пояснює нібито обмежене перетворення ALA в DHA збільшенням споживання омега-6. Вона також цитує дослідження з немовлятами, які свідчать про те, що харчова DHA є критично важливою для їхнього розвитку, — вона, як я зазначав вище, доступна через грудне молоко і не надає доказів еволюційної потреби в споживанні риби.
Ленґдон, 2006
У 2006 році Джон Ленґдон з кафедри біології та антропології Університету Індіанаполіса написав статтю — [Чи була дієта, заснована на фауні водойм, необхідною для еволюції мозку гомінідів і функціонального розвитку?], стверджуючи, що харчування продуктами фауни водойм не було критичним для еволюції людського мозку, а DHA не є важливою для розвитку мозку дітей сьогодні.
Ленґдон розглядає широкий спектр тем. Наприклад, він цитує опитування, яке виявило, що зі 123 сучасних груп мисливців-збирачів рибальство не забезпечувало суттєвої частини раціону в 23 групах.
На мою думку, цей уривок підсумовує найвагоміший аргумент Ленґдона:
“Загальний дефіцит [DHA] в організмі дозволяє замінити DHA іншими жирними кислотами в мембранах, включаючи докозапентаєнову кислоту (22:5n-6) [omega-6 DPA] або арахідонову кислоту (20:4n-6) [AA], щоб склад тканин тіла досить швидко змінювався, коли змінюється харчування (Neuringer та ін., 1988; Uauy, 1990; Neuringer, 1993). Ця заміна може бути тимчасовою, доки не відновиться рівень DHA в організмі, і це означає, що тимчасова нестача DHA необов’язково впливає на швидкість загального росту мозку.”
Давайте подивимося, які докази наводить Ленґдон на підтримку цієї точки зору.
Я не певен, для чого Ленґдон цитує [статтю Нойрінґера 1993 року]. У цьому короткому огляді Нойрінґер описує дослідження, в якому немовлята, яких годували сумішшю без DHA, мали нижчий рівень DHA (7,0-7,5%) у корі головного мозку порівняно з тими, хто отримував грудне молоко (~9,75%). Це сталося незважаючи на те, що одна група немовлят на штучному вигодовуванні була старшою (16-43 тижні), ніж немовлята на грудному вигодовуванні (5-16 тижнів), а DHA зазвичай накопичується в мозку з віком немовлят. У цьому дослідженні не розглядалося, чи можуть омега-6 DPA або AA адекватно замінити DHA, а отже не підтверджується аргумент Ленґдона.
Огляд 1988 року [Нойрінґера та ін.] здається більш доцільним в цьому сенсі. Дослідники стверджують:
“Як вперше спостерігали Mohrhauer & Holman, зниження DHA було компенсовано збільшенням n-6 жирних кислот 22:5n-6 і, меншою мірою, 22:4n-6. Отже, загальний рівень 22-вуглецевих поліненасичених жирних кислот залишався приблизно постійним, а ступінь поліненасиченості змінювався лише незначно. Це взаємне заміщення DHA довголанцюговими n-6 жирними кислотами є послідовним висновком у дослідженнях дефіциту n-3 жирних кислот. Це особливо вражає тим, що, за кількома винятками, 22:5n-6 зазвичай присутні у дуже низьких рівнях у тканинах тварин. Таким чином, співвідношення 22:5n-6 до 22:6n-3 у крові та тканинах було запропоновано як показник дефіциту n-3 жирних кислот [Galli et al., 1974].”
Neuringer та ін. стверджують, що заміщення DHA омега-6 DPA не є оптимальною. Серед їхніх джерел є дослідження [Mohrhauer and Holman (1963)] — там використовували щурів і не оцінювали жодних потенційних проблем із заміною DHA на довголанцюгові омега-6 жирні кислоти. Так само дослідження Galli та ін. використовували щурів і не оцінювали вплив заміщення DHA довголанцюговими омега-6 жирними кислотами.
Нарешті, [огляд Uauy 1990 року], цитований Ленґдоном, не надає доказів на підтримку твердження Ленґдона. Uauy фактично стверджує, що немовлятам потрібне харчове джерело DHA.
Хоча я прихильно ставлюся до більшої частини того, що пише Ленґдон, і хотів би, щоб це було правдою, найважливіша частина його статті мене не переконує.
Бердж, 2022
Грем Бердж є дослідником ліпідів з Університету Саутгемптона у Великобританії та був провідним дослідником серії досліджень перетворення омега-3 [Burdge et al., 2002] [Burdge and Wootton, 2002] [Burdge et al., 2003].
У 2022 році Бердж опублікував статтю — [Перетворення α-ліноленової кислоти є достатнім джерелом поліненасичених довголанцюгових жирних кислот ω-3 у людей]. У цій детальній оглядовій статті Бердж стверджує, що споживання ALA з їжею достатньо для задоволення потреб організму в EPA та DHA.
Замість занепокоєння тим, що вегетаріанцям може знадобитися прийом добавок DHA, Бердж стверджує, що, очевидно, здоров’я вегетаріанців і веганів, які тривалий час перебувають на рослинному харчуванні, свідчить про відсутність потреби в EPA та DHA.
Бердж каже, що при дефіциті омега-3 кислот омега-6 DPA накопичується у плазмових фосфоліпідах і що кілька досліджень вегетаріанців, в яких вимірювали рівні омега-6 DPA, не виявили накопичення. Бердж вказує на те, що [Sanders and Reddy (1992)] не виявили накопичення омега-6 DPA в еритроцитах немовлят, яких годували матері-веганки.
Однак Бердж не включає того висновку, що [Sanders and Reddy (1992)] також виявили у вегетаріанок-індуїсток більшу кількість омега-6 DPA в плазмі пуповини (2,34% проти 1,58%) і фосфоліпідах артерій (4,15% проти 3,19%) порівняно з всеїдними. Ці фракції не фіксувалися для веганок.
Вегетаріанки-індуїстки споживали ALA лише 0,9 г/день порівняно з 1,2 г/день для веганок. Хоча ця різниця невелика, 0,9 г/день є нижчим за рекомендовану добову норму омега-3 (від 1,1 до 1,4 г/день) і може бути достатньо низьким, щоб ці вегетаріанки мали дефіцит омега-3.
Бердж пише:
“Результати випробувань харчових добавок і експериментів з використанням стабільних ізотопних індикаторів були інтерпретовані як вказівки на те, що люди «погано» перетворюють [ALA], зокрема щодо синтезу DHA. Використання термінів «поганий», «обмежений» [або] суворо «обмежений» для опису синтезу полінасичених жирів у людей передбачає, що рівень перетворення має бути вищим, але яким має бути цей вищий рівень, не визначено та потенційно вводить в оману.
Радше наявну здатність до перетворення [ALA] у печінці людей краще розглядати як продукт еволюційної історії, а отже як адекватну з точки зору харчування.”
Висновок до еволюційних аргументів щодо харчових потреб у DHA
Еволюційні аргументи на користь харчових потреб у DHA цікаві, але докази здаються надто нечіткими, щоб розуміти, чи вони правдиві. На питання про те, чи потрібна сучасним людям DHA в раціоні для належного розвитку та підтримки мозку, можна відповісти лише за допомогою клінічних випробувань, які порівнюють результати у людей, які отримували та не отримували DHA з їжі.
Додаток C: Стеаринова кислота
Стеаринова кислота — це омега-3 з коротшим ланцюгом, яка є унікальною, оскільки не потребує того ферменту, що обмежує швидкість перетворення ALA в EPA. Є дуже небагато продуктів рослинного походження, які природним чином містять SDA, зокрема олії синяка подорожникового Echium plantagineum (echium) і горобейника польового Buglossoides arvensis (Ahiflower). Існують також генетично модифіковані соєві та рапсові олії, збагачені SDA.
Останнє оновлення у грудні 2022 року.
Бібліографія
___Omega-3s
by Jack Norris, RD, LD
Contents
EPA and DHA Correlate between Plasma and the Heart but not the Brain
Lower Omega-6 Intake is Associated with Higher Serum EPA and DHA
Appendix B: Evolutionary Arguments for a Dietary Requirement for DHA
Essential Information
Omega-3 fats are important for the long-term health of the heart and brain but are found in a limited number of plant foods. Walnuts, canola oil, flaxseeds and flaxseed oil, chia seeds, hemp seeds, and perilla oil are high in omega-3s.
A delicious way to get your daily omega-3s is from chia seed pudding, which you can eat for breakfast or as a dessert.
Chia Seed Pudding Recipe
In a bowl, whisk together:
1+3/4 cups of unsweetened non-dairy milk (or sweetened non-dairy milk and avoid the sweetener ingredient below)
1 to 2 tablespoons of sweetener (for example, sugar or maple syrup)
1/2 cup of chia seeds
1/2 to 1 teaspoon of vanilla extract (optional)
Chill for a few hours and stir before eating. The pudding is even better served with toppings, such as fruit, peanut butter, or chocolate chips. Keep refrigerated.

Another option is to keep a jar of hemp or ground flaxseeds in the refrigerator to sprinkle them on meals throughout the day—they’re easy to incorporate into anything you’re eating.
Dietary Reference Intakes for ALA
The table below lists the Dietary Reference Intakes (DRI) for the essential omega-3 fat, alpha-linolenic acid (ALA).
Plant Sources of ALA
Additional Tips
Whether vegans need to do more than meet the DRI for ALA for a normal omega-3 status is controversial (and discussed in great depth below).
To be extra cautious, vegans can take one of these additional steps:
Consume an additional 2,000 mg of ALA per day using the foods in the table above.
Take a supplement of 200-300 mg of DHA per day.
Your DHA supplement can contain EPA, but it’s not necessary to contain EPA if you’re meeting the DRI for ALA. We don’t recommend or have opinions on any specific brands of DHA supplements.
Too much omega-3 can result in bleeding and bruising. If you bleed or bruise easily, consult a health professional before significantly increasing your omega-3 intake.
See below for our recommendations for pregnancy, nursing, and infants.
Flax
If flaxseeds are not ground, they will not be digested [Austria, 2008]. They can be ground in a blender (works best with a large amount) or coffee grinder, and then stored in the freezer. Ground flaxseeds can be sprinkled on cereal or used in baked goods.
There is some evidence that people 45 and older do not absorb the oil from ground flaxseeds as well as from flaxseed oil [Patenaude, 2009]. The one study indicating this was only for four weeks and used 6 g of ALA per day. With smaller amounts and for longer periods, the difference might be negligible, but that hasn’t been tested.
Cooking flaxseed oil damages the ALA, but it can be put on warm food such as toast.
Flaxseed oil should be kept in the refrigerator.
Flaxseed oil doesn’t taste very good. Some people use cinnamon-flavored oil, tablets, or put it on toast or salad to disguise the taste.
Research on Omega-3 Fatty Acids in Plant-Based Diets
There are two questions regarding vegetarians and omega-3s: Do vegetarians have negative health consequences from not eating fish and should vegetarians supplement with the omega-3s found in fish (EPA and DHA)? Although vegetarians and vegans have been shown in many studies to have lower blood levels of EPA and DHA than fish-eaters, the quick answer to these questions is that there isn’t sufficient evidence to conclude that the lower levels have negative health consequences.
The rest of this article discusses the arguments and research surrounding this issue.
Background on Omega-3s
For our purposes, there are four important omega-3 fatty acids:
alpha-linolenic acid (ALA) • Short-chain (18 carbon) omega-3 fatty acid. Found in small amounts in animal flesh, in very small amounts in a variety of plant products, and in relatively large amounts in soy, walnuts, canola oil, flaxseeds and their oil, hempseed oil, camelina oil, perilla oil, and chia seeds. The human body cannot make its own ALA; it must be obtained through the diet.
eicosapentaenoic acid (EPA) • Long-chain (20 carbon) omega-3 fatty acid. Found mostly in fatty fish, in small amounts in eggs, and in very small amounts in seaweed that can be concentrated into supplements. Some EPA is converted into series 3 eicosanoids which can reduce blood clotting, inflammation, blood pressure, and cholesterol. The human body can produce EPA from ALA and possibly from DHA.
docosapentaenoic acid (DPA) • Long-chain (22 carbon) fatty acid. There is both an omega-3 and omega-6 version of DPA. The omega-3 version is an intermediary between EPA and DHA.
docosahexaenoic acid (DHA) • Long-chain (22 carbon) omega-3 fatty acid. Found mostly in fatty fish, in small amounts in eggs, and in very small amounts in seaweed that can be concentrated into supplements. DHA is a major component of the gray matter of the brain, and also found in the heart, retina, testis, sperm, and cell membranes. The body can convert EPA into DHA.
The chart below shows the conversion pathways for the omega-3 and omega-6 fatty acids. In the chart, D6D is the enzyme that converts ALA and LA into other fats.

See the video below for an excellent overview of omega-3 fatty acids from omega-3 researcher Dr. Richard Bazinet of the University of Toronto (2021).
[[VIDEO https://www.youtube.com/watch?v=fPkx8U9f-dI ]]
Essential Fatty Acid Intakes of Vegans
The Institute of Medicine considers there to be a dietary requirement for two fatty acids for people age 1 year and older, alpha-linolenic acid (ALA) and linoleic acid (LA). However, [Burdge (2022)] reports that an overt deficiency of ALA has never been fully isolated from LA and fat-soluble vitamin deficiencies in adult humans in order to clearly demonstrate that ALA is an essential fatty acid.
The table below shows the weighted averages of studies measuring vegan ALA intakes. Calculations and citations are in our ALA Intakes spreadsheet.
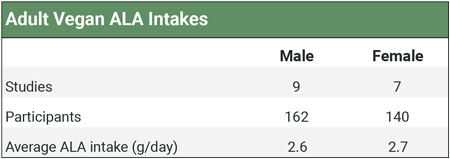
The [World Health Organization and Food and Agriculture Organization (2010)] recommend an LA intake between 2.5% to 9% of calories, saying that the lower number prevents deficiency and the higher end of the range reduces the risk for heart disease.
Although vegans who don’t ensure sources of ALA tend to have a high ratio of omega-6 to omega-3 fats, their percentage of calories as LA has been shown to be 5.1% [Pinto, 2017, United Kingdom], 7.3% [Allès, 2017, France], 8.5% [Kornsteiner, 2008, Austria], and 9.3% [Rizzo, 2013, USA], well within the range recommended by the WHO.
Long-chain Omega-3 Fatty Acid Blood Levels of Vegetarians
Summary: The differences in long-chain omega-3 blood levels between vegans, lacto-ovo-vegetarians, and omnivores aren’t obviously physiologically significant, especially with regard to omnivores who don’t regularly eat fish. Red blood cell DHA of vegetarians and vegans is roughly 72-75% of that of omnivores, but it’s not clear if this has clinical significance.
There is no standardized method for measuring omega-3 fatty acids: no one knows what levels of fatty acids in any given medium represent a deficient, healthy, or optimal level. It could even be that blood levels of fatty acids have little bearing on omega-3 fatty acid status. The purpose of this section is to determine whether vegans do indeed have lower blood levels of long-chain omega-3 fatty acids than omnivores. Early studies found that vegans have lower EPA and DHA blood levels, but these studies were conducted on very few people; more recent studies haven’t shown nearly the difference.
As of early 2022, we’ve tracked 27 studies measuring the blood levels of omega-3 fatty acids in vegetarians. We list these studies and their measurements in the Cross-sectional tab of our spreadsheet, Omega-3s Part 2: Research.
The way omega-3s are measured among these studies varies considerably.
Fatty acids can be measured in various components of plasma such as phospholipids, triglycerides, or cholesterol esters. Fatty acids may also be measured in the adipose tissue, platelets, or red blood cells. Because red blood cells have a lifespan of 120 days, red blood cell fatty acids might be a more accurate long-term representation of omega-3 status.
In the plasma, omega-3s are usually measured as a percentage of total fatty acids, but [Welch et al. (2010)] measured omega-3s as a concentration in plasma and [Rosell et al. (2005)] provided the data to calculate a concentration. Concentrations might be a more accurate reflection of the body’s omega-3 stores since they represent an absolute rather than a relative amount.
DPA is a long-chain omega-3 fatty acid that is an intermediary between EPA and DHA. We emphasize studies that included DPA in their measurements because DPA represents a significant fraction of long-chain omega-3s that vegans have converted from ALA and which can potentially be converted to DHA.
The graph below plots all measurements that compared total long-chain omega-3 levels (EPA+DPA+DHA) of vegetarians or vegans to omnivores. It includes measurements of percentages and concentrations for each medium. While there’s considerable overlap between diet groups, individual studies generally find that omnivores have higher levels of long-chain omega-3s than vegans with the differences being statistically significant.
 of vegetarians or vegans to omnivores")
The graphs below compare only the EPA or DHA levels of vegans and vegetarians in all studies that measured EPA or DHA.


Arguably the most important metric is red blood cell omega-3s, shown in the graph below.

It’s hard to conclude much regarding vegan long-chain omega-3 levels from these studies given that the measurements aren’t standardized, aren’t well understood, and contain significant overlap. Arguably a more accurate way to assess this data is to weight the comparisons of vegetarians both proportional to the omnivores in the same studies and proportional to how many people were in each diet group while limiting the measurements to one per population studied.
In order to get the most accurate picture of how long-chain omega-3 blood levels of vegans compare to those of omnivores, we decided to calibrate the measurements by creating a ratio of the levels of vegans to those of omnivores rather than using an absolute amount. We did this by simply dividing the vegan level by the omnivore level.
For example, the study by [Kornsteiner et al.] found an EPA+DPA+DHA percentage of total fatty acids in red blood cells of 1.96% for vegans and 3.34% for omnivores. The study by [Li et al.] found an EPA+DPA+DHA percentage of total fatty acids in plasma of 3.6% for vegans and 5.5% for omnivores. We don’t know if we can compare the percentage of fatty acids in red blood cells to the fatty acids in plasma, but we can compare the ratio of vegan to omnivore long-chain omega-3s in both studies, which was .59 in Kornsteiner et al. and .65 in Li et al.
We can then multiply these two ratios by the number of vegans in their respective study, divide by the total number of vegans in both studies, and get a weighted average of the ratio of vegan to omnivore long-chain omega-3s across both studies. By weighting all of the studies in this way, we can obtain the most accurate picture of how blood levels of long-chain omega-3 fatty acids compare for vegans and omnivores.
Most studies measured omega-3s as a percentage of total fatty acids; to be as consistent as possible, we weighted the percentage of total fatty acids rather than the concentration for studies that measured both. For studies with multiple measurements, we chose in this order: red blood cells, plasma, platelets, and adipose tissue.
The table below shows the weighted proportions of omega-3s for vegetarians and vegans compared to omnivores for all studies and for red blood cell (RBC) measurements only. Calculations and citations are in the Cross-sectional tab of our spreadsheet, Omega-3s Part 2: Research.
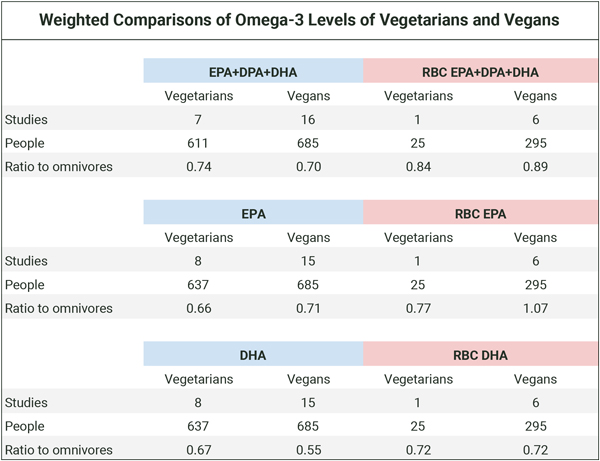
Based on the table above, vegans generally have lower blood levels of long-chain omega-3s than omnivores. Since plasma levels of omega-3s are at least in part a representation of dietary fatty acids, as distinct from representing only the body’s ability to convert dietary short-chain to long-chain omega-3s, it’s not surprising that people who have an intake of long-chain omega-3s have higher blood levels.
Vegetarians vs. Fish-Eaters
Among people who don’t supplement with long-chain omega-3s, regular fish-eaters will be the only dietary group with a significant source of long-chain omega-3s. According to the USDA nutrient database, a medium egg contains about 2 mg of EPA and 16 mg of DHA. That provides lacto-ovo-vegetarians with very small amounts of dietary EPA and DHA.
There are two studies that measured omega-3 levels among fish-eaters [Welch, 2010] [Miles, 2019], but neither measured it in red blood cells. We analyze these studies in the Fish-eaters tab of our spreadsheet Omega-3s Part 2: Research and summarize the results in the three charts below. Participants in the studies didn’t use long-chain omega-3 supplements.
[Welch, 2010] measured omega-3 plasma concentrations and separated omnivores into groups who did and did not eat fish. There were only 10 vegans.
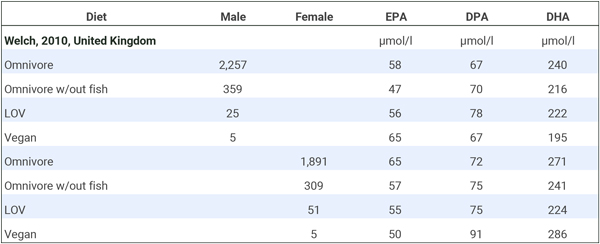
We combined the male and female long-chain omega-3 plasma concentrations to determine how vegans compared to both fish-eating and non-fish-eating omnivores. Because there were so few vegans, we also combined the lacto-ovo-vegetarians (LOV) with the vegans for a “vegetarian” category. The table below shows that lacto-ovo-vegetarians, vegans, or the combined group had levels slightly below fish-eaters and either similar or higher levels than non-fish-eaters.
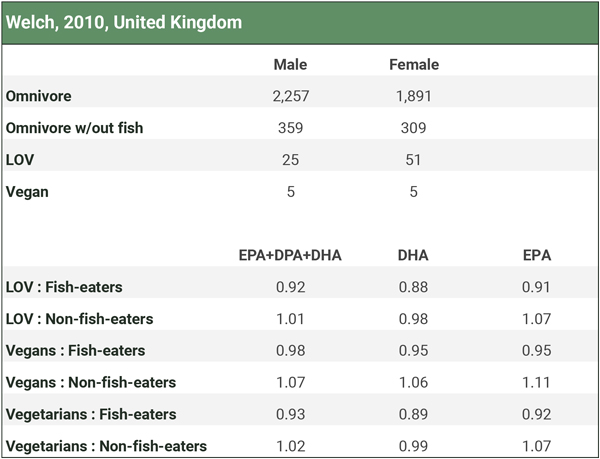
[Miles, 2019] compared the percentage of omega-3 fatty acids in the adipose tissue of pescatarians to other dietary groups, as shown in the table below. Vegetarians and vegans had lower levels than omnivores and even somewhat lower levels than fish-eaters. Although vegans had substantially lower levels than fish-eaters in this study, it’s not clear what the percentages of fatty acids in adipose tissue represent; possibly nothing of clinical significance.
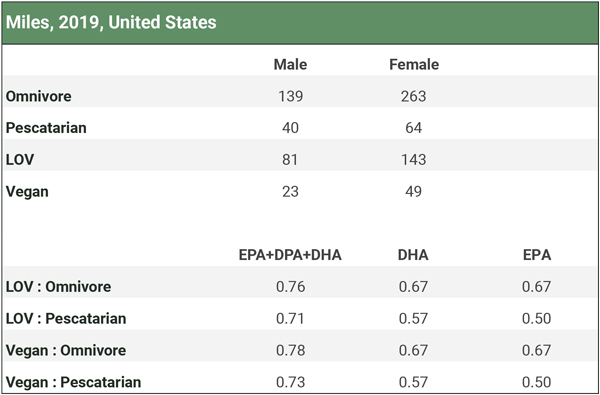
Fatty Acid Levels of Older vs. Younger Vegans
It’s normally thought that people have a harder time converting ALA to EPA and DHA as they age. [Sarter et al. (2015)] found that 69 vegans aged 60 to 85 had EPA+DHA levels of about 4.0% compared to about 3.6% for 97 vegans aged 20 to 59 (p for trend = 0.009).
Impacts of Lower EPA and DHA on Vegetarians
A possible benefit of long-chain omega-3 fatty acids, especially EPA, is to reduce blood clotting which protects against heart attacks. There have been some differences noted in blood clotting between vegetarians and omnivores.
[Mezzano et al. (1999, Chile)], found that vegetarians had significantly more platelets (242,000 per ul) than non-vegetarians (211,000 per ul) and a shorter bleeding time (4.5 vs. 7.3 min), which could increase the risk of a cardiovascular event. In a follow-up study, [Mezzano et al., 2000, Chile)] gave vegetarians 700 mg EPA and 700 mg DHA for 8 weeks. EPA went from .2 to 1.8% and DHA went from 1.1 to 3.0%. Some clotting factors changed, but bleeding time remained lower at 5-1/2 minutes.
[Sanders and Roshani (1992, United Kingdom)] found that one of eight platelet aggregation parameters in vegan men, but not women, was different from the non-vegetarians. Bleeding times were similar.
[Pinto et al. (2017, United Kingdom)] compared heart rate variability between a group of 23 adult vegans and 24 omnivores. Low heart rate variability reflects a reduced capacity for the heart to respond to the body’s physiological demands and is linked to an increased risk for heart disease. As expected, the vegans had lower concentrations of DHA and EPA in both red blood cells and plasma. While vegans had a higher heart rate variability over a 24-hour period, their daytime heart rate variability was lower, and their heart rate was greater. The clinical significance of these findings aren’t clear.
Thus, of three studies that looked at cardiovascular markers, the results are mixed.
In terms of cognition, in their study of British mortality, [Appleby et al. (2002)] found vegetarians to have a barely statistically significant, higher risk of death from mental and neurological diseases (DRR 2.21, CI 1.02–4.78).
In contrast, a more recent report from EPIC-Oxford [Appleby, 2016] found that vegetarian deaths from mental and behavioral disorders were not statistically different from non-vegetarians (HR 1.22, CI 0.78–1.91). And a report from the Adventist Health Study-2 [Orlich, 2013, USA] found no difference in mortality from neurologic diseases between vegetarians and non-vegetarians (HR 0.93, CI 0.67-1.29); pescatarians and semi-vegetarians were included in their vegetarian category so the results can’t be extrapolated to vegetarians who don’t eat fish.
Conversion of ALA to EPA and DHA
Measurements of the percentage of total fatty acids as EPA and DHA in the blood are generally considered a marker of omega-3 status. This assumes that higher percentages of total fatty acids in the blood reflect higher and more optimal amounts in the tissues that utilize omega-3s. It also assumes that when blood percentages change due to changes in dietary intake, levels in tissues respond similarly.
In this section, we examine these assumptions. Evidence of omega-3 conversion enzymes in tissues and down-regulation of omega-3 conversion in response to dietary omega-3s suggest that the body can regulate the conversion of omega-3 fatty acids in tissues independent of the percentage in the blood.
There’s evidence that high intakes of EPA and DHA will increase their percentages in both blood and tissues, but it’s not clear if higher percentages are necessary for optimal health. We assess the evidence in our sections Impacts of Lower EPA and DHA on Vegetarians and Omega-3s and Chronic Disease.
ALA Supplementation Results in Little Increase in Blood DHA
Our ALA Trials spreadsheet lists a handful of clinical trials, including all of the trials with vegetarians of which we’re aware, investigating whether increasing dietary ALA subsequently increases the percentage of long-chain omega-3s in the blood. The changes in total fatty acids as long-chain omega-3s show a wide variation with no clear pattern; some even found a decrease in DHA. On average, EPA+DPA+DHA increased by 43.5% while DHA only increased by 4.6%.
It’s safe to say that supplementing with ALA is unlikely to substantially increase the blood percentage of fatty acids as DHA in most adults.
EPA and DHA Correlate between Plasma and the Heart but not the Brain
Summary: Based on limited, mostly cross-sectional data, there appears to be a robust correlation between the blood and tissue percentages of EPA+DHA in the human heart but not the brain or sperm.
Studies of ALA supplementation result in very little increase of DHA in the blood, but how much evidence is there to suggest that this reflects the body’s inability to convert ALA to DHA for tissue utilization?
A basic question is, without any dietary changes, how much do blood levels of omega-3 fatty acids typically correlate with tissue levels? It’s difficult to study the omega-3 content of tissues in living humans. In our spreadsheet, Tissue Correlations, we list the correlations between blood and tissue percentages of omega-3s in both humans and animals. A summary of the results follows.
[Harris et al. (2004)] measured the correlation between the percentage of EPA+DHA in red blood cells and the percentage of EPA+DHA in the hearts of 20 heart transplantation patients having routine heart biopsies, 13 of whom were considered to be high consumers of EPA and DHA; they found a statistically significant, strong correlation (R = 0.82, P ≤ 0.0001).
[Harris et al. (2004)] also performed an intervention: Heart transplantation patients (n=25) with low EPA+DHA intakes were provided 1,000 mg of EPA+DHA for 6 months. These patients had weaker correlations between red blood cell and heart EPA+DHA at baseline (R = 0.47, P = 0.031). Post-intervention measurements showed that EPA+DHA percentages increased in plasma, red blood cells, heart, and cheek tissue; the correlation between red blood cell and heart EPA+DHA remained the same (R = 0.47, P = 0.06).
[Metcalf et al. (2007)] placed a series of patients on ALA (5.8 g per day) or EPA+DHA (6.3 g, ~50% each) for a number of weeks based on their heart surgery schedule. While they didn’t test for a correlation between red blood cell and heart omega-3 fatty acid percentages, the percentages of the two mediums were fairly similar and differed from the control group in similar amounts post-treatment (see our spreadsheet ALA Trials).
[Cunnane et al. (2012)] performed autopsies on cognitively normal people and found a correlation between percentages of DHA in plasma phosphatidylethanolamine and the angular gyrus region of the brain DHA (R = 0.77, P ≤ 0.005). However, they failed to find correlations between DHA and other regions or in cognitively impaired people stating, “No significant correlations were observed for DHA (% or mg/g) or any other fatty acids in the other brain regions or in the [Alzheimer’s disease] and [mildly cognitively impaired] groups (data not shown).”
[Carver et al. (2001)] performed autopsies on 58 people and found a negative correlation between the DHA percentage in red blood cells and the cerebral cortex of people aged >18 years; it’s likely this correlation doesn’t achieve statistical significance after a Bonferroni correction for the large number of correlations tested.
[Chamorro et al. (2020)] measured the fatty acid percentages of young men, comparing vegans (n=34) and omnivores (n=33). They didn’t test for a correlation between the percentage of omega-3s in plasma or red blood cells and sperm. The ratio of the percentage of EPA in sperm to that in plasma and red blood cells was similar at 0.54 for each, but the ratios for DPA and DHA were not. See the table below.
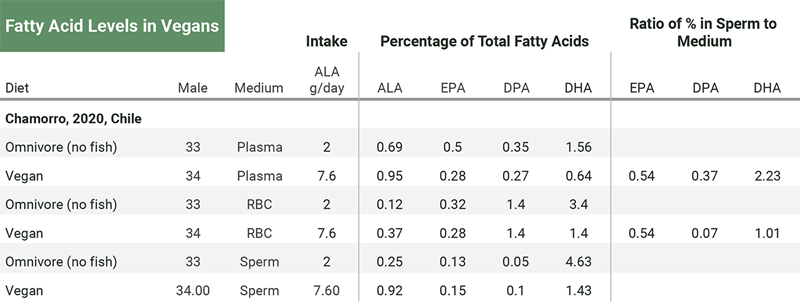
There’s much more data from animals than humans. Our spreadsheet, Tissue Correlations, lists 24 correlations between blood and tissue percentages of EPA+DHA among rats, pigs, and mice. The strength of the correlations varies considerably with some being negative.
There’s one other study on animals worth mentioning. [Talahalli et al. (2010)] fed two groups of rats a reasonable amount of ALA (2.5% and 5.0% of calories). After 60 days, the percentage of fatty acids as DHA in the brain of the rats fed 2.5% and 5.0% ALA was, respectively, 9.4% and 10.4% compared to 8.3% in the control group (see the table, Talahalli 2010). This suggests that ALA supplementation increased the amount of DHA in their brains.
One significant caveat for comparing the conversion of omega-3s in rats, pigs, and mice to humans is that rats, pigs, and mice normally don’t have a dietary source of EPA or DHA and, therefore, would normally rely entirely on the conversion from ALA for any EPA or DHA.
While plasma and red blood cell percentages of long-chain omega-3 fatty acids sometimes correlate with tissues, they don’t do so consistently. It might be possible to develop a mathematical model that can account for the large number of variables that impact the correlations but it seems unlikely that a model will be developed that gives us confidence in predicting the omega-3 tissue status of vegetarians.
In Appendix A, we discuss a review paper, Biomarkers of DHA status, arguing that blood percentages are adequate markers of DHA status.
Tissues Contain Enzymes that Convert Omega-3s
Two critical enzymes, delta-5 desaturase and delta-6 desaturase, convert short-chain omega-3 and omega-6 fatty acids into long-chain versions.
Previously, the liver was considered the primary site of EPA and DHA production for peripheral tissue utilization, but studies by [Cho et al., 1999a] and [Cho et al., 1999b] found substantial amounts of mRNA for the delta-5 and delta-6 desaturase enzymes in many tissues of human cadavers.
[Cho et al., 1999a] found that delta-5 desaturase mRNA was greatest in the human liver, but that the heart, brain, and lung also contained substantial amounts. They found low but detectable levels in the placenta, skeletal muscle, kidney, and pancreas. [Cho et al., 1999b] found that the amount of delta-6 desaturase mRNA in the human liver was comparable to that found in the human lung and heart, while the adult brain had a level several times greater than the liver.
[Cho et al., 1999a] point out that the expression of these enzymes can vary greatly among individuals. The authors hypothesize that this might be due to age or, more likely in their view, regulation of the enzymes in response to the dietary intake of fatty acids.
Using cross-sectional data based on the percentage of plasma phospholipids, [Welch et al. (2008, United Kingdom)] estimated that non-fish-eaters (both vegetarians and meat-eaters) converting to long-chain omega-3s at about a 22% higher rate than fish-eaters.
Dietary DHA Reduces ALA Conversion
In a series of three studies, researchers used a carbon tracer to track the conversion of a 700 mg dose of ALA to long-chain omega-3s in the blood of three different groups of people. The results are in the table below. Only females (all of whom were of reproductive age) showed a substantial conversion of ALA to DHA in the blood.
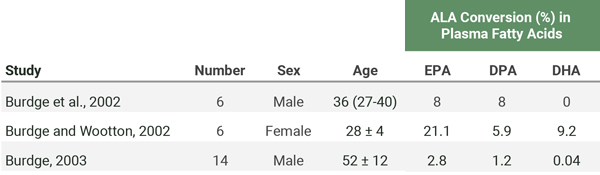
In addition to the baseline measurements listed in the table above, [Burdge et al. (2003)] included an 8-week intervention on three groups of older men: a control group (n=5), a group whose daily ALA was increased from their normal intake of 1.7 g to 10 g (n=4), and a group whose daily EPA+DHA was increased from their normal intake of 264 mg to 1.6 g (n=5). After 8 weeks, they fed each person 700 mg of ALA with a carbon tracer and found that the ALA supplemented group’s conversion of ALA to long-chain omega-3s hadn’t increased whereas the EPA+DHA supplemented group’s conversion had decreased.
[Vermunt et al. (2000)] fed carbon-labeled ALA to humans and found that the conversion of ALA to EPA, DPA, and DHA was much greater after 9 weeks of a diet high in oleic acid compared to after a diet high in ALA or EPA+DHA.
The two trials mentioned above by [Burdge et al. (2003)] and [Vermunt et al. (2000)] suggest that there’s a down-regulation of ALA conversion to long-chain omega-3s in humans who have a regular supply of ALA or EPA and DHA. The simplest explanation for this down-regulation is that their tissues had sufficient long-chain omega-3 levels.
Further evidence for enzymatic regulation due to dietary intake is a study by [Metherel et al. (2019)] who conducted a randomized controlled trial using carbon-labeled DHA. While plasma levels of EPA increased, it wasn’t due to DHA being converted to EPA, suggesting that the dietary supply of DHA resulted in the down-regulation of the conversion of EPA to DHA.
[Burdge and Wootton’s (2002)] data showed an uneven distribution of omega-3 fatty acids among the different components of plasma lipids (cholesterol esters, phosphatidylcholine, triglycerides, and non-esterified fatty acids). They surmised that plasma cholesterol esters act as a long-term source of ALA within circulation that may provide tissues containing active desaturation and elongation pathways (brain, heart, and skeletal muscles) a steady source of ALA for conversion to EPA, DPA, and DHA while tissues with low expressions of these enzymes, such as the kidney and pancreas, may be dependent upon the supply of pre-formed EPA, DPA, and DHA.
Lower Omega-6 Intake is Associated with Higher Serum EPA and DHA
The traditional way vegetarians have been encouraged to raise blood EPA and DHA levels is by increasing ALA and decreasing the omega-6 fatty acid, linoleic acid (LA). This is because the enzymes that convert ALA into EPA and DHA also convert the omega-6 fatty acids and there is competition for these enzymes. Some evidence for this theory is from a clinical trial by [Liou et al. (2007, Canada)] who found increasing LA intake resulted in a lower percentage of EPA in plasma phospholipids
Most vegetable oils are high in omega-6s and vegetarians tend to get plenty in their diets. [Sanders and Younger (1981, United Kingdom] found a dietary ratio of omega-6s to omega-3s of 16 for vegans and 6 for meat-eaters. [Sanders and Roshanai (1992, United Kingdom)] found a dietary ratio of 15.8 for vegan men, 10.2 for meat-eating men, 18.3 for vegan women, and 8.2 for meat-eating women.
There are no clinical trials that increase the ALA intake of vegetarians while also decreasing their LA intake, to see what impact this has on blood levels of EPA and DHA.
[Salvador et al. (2019, Spain)] studied 55 vegans and 49 lacto-ovo-vegetarians and found that those with a serum omega-6 to omega-3 ratio of ≤ 10 had a higher percentage of serum EPA and DHA than those with a ratio between 10 and 20 or >20 (EPA: 0.60%, 0.27%, and 0.23%; DHA: 2.90%, 1.91%, and 1.19% respectively). Flaxseed intakes of once per day and, especially, 2 or more times per day were associated with a much higher percentage of serum ALA (~0.5% vs. ~0.7% and 1.5%, respectively), but not with higher EPA or DHA percentages.
Based on limited research, lowering LA intake could increase blood levels of long-chain omega-3s, but it’s not known if doing so impacts tissues or provides health benefits.
Low Omega-6 to Omega-3 Ratio Foods
At this time, the research indicates that vegetarians with lower dietary omega-6 to omega-3 ratios tend to have higher blood levels of EPA and DHA. For that reason, it’s prudent, when adding ALA to the diet, to choose foods that don’t also substantially increase omega-6 intake, listed in the table below.
DHA Supplementation in Vegetarians
Studies consistently show that supplementing vegetarians and vegans with DHA from algal sources increases their blood percentage of DHA [Sanders, 2009] [Geppert, 2006] [Wu, 2006] [Conquer, 1996] [Conquer, 1997]. Studies also show that supplementing with both EPA and DHA increases vegetarians EPA and DHA percentages [Sarter, 2015] [Mezzano, 2000].
Fish contains about twice as much DHA as EPA [Kris-Etherton, 2009], so it’s not unusual for fish-eaters to eat more DHA than EPA. [Conquer and Holub (1996, Canada)] showed an 11–12% increase in EPA after 6 weeks of 1,620 mg of DHA in vegetarians.
Upon DHA supplementation, EPA levels also increase by a small percentage. Using a carbon tracer, [Brossard et al. (1996, France)] found a 1.4% conversion of DHA to EPA in three people given one dose of 123 mg of DHA over the course of 20 hours. In contrast, [Metherel et al. (2019, Canada)] conducted a randomized controlled trial using DHA containing labeled carbon and didn’t find any to be converted to EPA. They conclude that “the increase in plasma EPA following DHA supplementation in humans does not occur via retroconversion, but instead from a slowed metabolism and/or accumulation of plasma EPA.”
Omega-3 Recommendations for Vegans
To sum up the rationale behind our recommendations, it appears that if a vegan is meeting the Dietary Reference Intake for ALA, their EPA status should be adequate. To be cautious we recommend either increasing ALA intake or adding a DHA supplement. Please see our article, Daily Needs, for specific recommendations and how to meet them.
There are many vegan DHA and EPA supplements available via the Internet. We aren’t able to assess whether any given company is better than another.
Vegetarian Pregnancy, Nursing, and Infants
This section provides our omega-3 recommendations for vegetarians and vegans, followed by a discussion of the state of the research.
Summary and Recommendations
The United States and Canadian Dietary Reference Intakes don’t specifically recommend a DHA supplement during pregnancy or lactation. Their recommendations are for an extra 300 mg of ALA during pregnancy (for a total of 1.4 g/day) and an extra 200 mg of ALA during nursing (for a total of 1.3 g/day). Their recommendations for non-breastfeeding infants is for an infant formula with 500 mg of total omega-3s (ALA, EPA, and DHA) per day [National Institutes of Health, 2022].
However, a number of organizations have superseded the DRIs by specifically recommending DHA for the general public during pregnancy and/or nursing, including the International Society for the Study of Fatty Acids and Lipids (ISSFAL) and the American Academy of Pediatrics (AAP).
The most recent Cochrane analysis of randomized controlled trials found a benefit of DHA supplementation in preventing early preterm births among apparently healthy, pregnant women [Middleton, 2018]. At VeganHealth, the purpose of our recommendations are for preventing nutrient deficiencies more than for treating disease.
The finding that DHA reduces the risk of a small percentage of preterm births is possibly due to a therapeutic effect of DHA rather than from correcting a nutrient deficiency. If this is the case, then meeting the DRIs for ALA might prevent an omega-3 deficiency during pregnancy and nursing, but without more research, erring on the side of caution is prudent.
Our recommendations for pregnancy, nursing, and infants are:
Maternal diet during pregnancy
Meet the DRIs for ALA of 1.4 g per day (see Daily Needs for sources).
Supplement with 300-600 mg of DHA per day [Carlson, 2013] [Harris, 2015].
Maternal diet during nursing
Meet the DRIs for ALA of 1.3 g per day (see Daily Needs for sources).
Evidence isn’t convincing for DHA supplementation, but some organizations recommend at least 200 mg per day [Koletzko, 2007] [Meek and Noble, 2022].
Formula-fed infants
Use a formula with 500 mg of total omega-3s (ALA, EPA, and DHA) per day; EPA and DHA are not specifically required if there’s 500 mg of ALA.
Children eating only solid food
Meet the DRIs for ALA (see Daily Needs for amounts and sources).
Research on Pregnant and Nursing Vegans
[Ureta-Velasco et al. (2023, Spain)] compared the breast milk of 20 vegetarians (including 11 vegans) to that of omnivores. The authors describe their study as one of the most complete investigations available due to having a 5-day dietary record, multiple milk samples from each participant, and measuring plasma levels of nutrients. However, the study was conducted to determine the quality of breast milk of vegetarians for donation purposes and the milk was processed and stored as donated breast milk would be; the authors said this made the results “not superimposable” to those of breast milk fed directly to infants.
Intakes of ALA were 1.58 g/day for meat-eaters and 2.24 g/day for vegetarian mothers. Among the vegetarian group, 30% had used omega-3 supplements during pregnancy and 35% were using during lactation. Total EPA plus DHA intake, including from supplements, was .53 g/day for omnivores and .14 g/day for vegetarians. Shown in the chart below, DHA in the vegetarians’ erythrocytes, plasma, and breast milk was significantly lower.
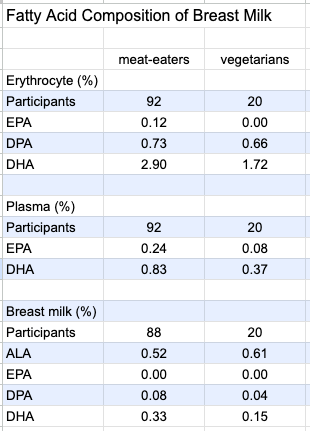
The authors write:
“However, we do not consider this to be a reason for the exclusion of vegetarian/vegan women as milk donors. Firstly, the intakes and levels of DHA in human milk vary widely across countries. Indeed, values equal or even lower than those of our Veg group have been reported both in developed and developing countries. In fact, several studies on [donor human milk] in North America found DHA values that were similar to or even lower than those of our Veg group. Secondly, since DHA supplementation to lactating women has consistently been shown to increase DHA concentrations in breast milk, it seems an appropriate strategy to recommend DHA supplementation from algal oil to Veg women who want to become milk donors.”
[Specker et al. (1987, USA)] compared the fat content of the breast milk of 7 nonvegetarian women to 12 women on a macrobiotic diet (mostly vegan with some occasional animal foods including seafood). The percentage of fat as DHA in the women’s breast milk was similar (0.27% for the macrobiotic women and 0.29% for the nonvegetarians).
[Reddy and Sanders (1994, United Kingdom)] measured the DHA levels in the umbilical cords of 32 infants born to Hindu vegetarian mothers living in North London and compared them to omnivores. The vegetarians had a lower percentage of DHA cord plasma phospholipids (4.0% vs. 5.8%) and cord artery phospholipids (4.1% vs. 5.8%). The Hindu vegetarian infants were born with lower body weight, length, and head circumference but there was no relationship between those parameters and the percentages of DHA in their cord plasma or cord artery phospholipids.
[Reddy and Sanders (1994, United Kingdom)] also measured the percentage of fat as DHA in the breast milk of 19 vegans (0.14%), 5 vegetarians (0.30%), and 21 omnivores (0.37%).
[Perrin et al. (2018, USA)] found that the ALA in breast milk was significantly higher in vegans (2.1%) than vegetarians (1.4%) and meat eaters (1.2%). They found no statistically significant differences between the DHA levels in 26 vegans (0.14%), 22 vegetarians (0.17%), and 26 meat-eaters (0.18%). DHA was undetectable in 14.9% of samples; there was no difference in the prevalence of undetectable samples between the diet groups.
The authors note:
“Two independent reviews of worldwide DHA breast milk concentrations reported averages of 0.32–0.37%, with concentrations in US populations often reported at 0.20% or lower, which is similar to our findings. While use of a DHA supplement is well supported in the literature as a way to increase breast milk DHA, less than one-third of vegans in our study reported using DHA supplements. Similarly, fish consumption was low, with only 3/26 (11.5%) of omnivores and 0/22 (0.0%) vegetarians reporting more than weekly consumption.”
Because term infants as young as 3 weeks can convert ALA to DHA [Sauerwald, 1996], it’s not clear if lower percentages of DHA in vegan breast milk are of physiological significance.
Research on Omega-3 Supplementation in Pregnancy, Lactation, and Infancy
Dozens of clinical trials have measured the impact of DHA supplementation on infant development. Some studies provide DHA directly to the infants while others provide the DHA to their pregnant or nursing mothers.
There are two large systematic reviews on the topic:
Omega-3 Fatty Acids and Maternal and Child Health: An Updated Systematic Review [Newberry et al., 2016], prepared for the Agency for Healthcare Research and Quality (AHRQ) of the U.S. Department of Health and Human Services. This over 800-page report provides an analysis of 95 randomized controlled trials and 48 observational studies.
Omega-3 Fatty Acid Addition during Pregnancy [Middleton, et al., 2018], a Cochrane Database Systematic Review. This over 400-page report provides an analysis of 70 randomized controlled trials.
They come to somewhat different conclusions, especially regarding the risk for preterm births.
The AHRQ report [Newberry et al., 2016] found that evidence was sufficient to draw a conclusion of low or moderate strength for the following outcomes:
Supplementation with DHA increased the length of gestation but didn’t decrease the risk for preterm birth.
Prenatal DHA supplementation increased the birth weight among healthy term infants but didn’t decrease the risk for low birth weight.
Prenatal DHA supplementation didn’t increase the risk of gestational hypertension or preeclampsia among high-risk women.
DHA supplementation did not impact post-delivery infant growth patterns (weight, length, or head circumference).
Prenatal supplementation with DHA had no effect on visual acuity.
For term infants, data conflicted on the effectiveness of supplementing infant formula with omega-3 fatty acids depending on when and how the visual acuity was assessed and the type of omega-3 provided.
Omega-3 supplementation had no consistent effect on neurological development.
Supplementing or fortifying infant formula for term infants with omega-3s had no effect on cognitive development.
Omega-3 supplementation had no effect on the development of autism spectrum disorder, attention deficit hyperactivity disorder, atopic dermatitis, allergies, or respiratory disorders.
Maternal DHA or EPA supplementation had no effect on the risk of peripartum depression.
The authors couldn’t rule out the possibility that supplementation can help those at higher risk of poor outcomes or people with low DHA levels at baseline:
“Few studies stratified outcomes according to risk groups, so it was usually not possible to assess whether the effectiveness of omega-3 interventions depended on level of risk. In addition, no RCTs stratified outcomes by baseline n-3 FA status, so it is not possible to assess whether adequacy of n-3 FA status might account for differences in outcomes across (or lack of outcomes within) studies.”
The Cochrane Database review [Middleton, 2018] found few statistically significant impacts of omega-3 supplementation except for a reduced risk of preterm births and low birth weight. Non-statistically significant trends were for supplementation to reduce the risk of perinatal infant death and neonatal care admission, and an increased risk of large-for-gestational-age babies. We’ll discuss the preterm births < 34 weeks in more detail as it was the most promising finding.
Long-chain Omega-3s and Preterm Births
The Cochrane report found a lower risk of preterm bir Middleton, 2018). The report included at least one study that used ALA rather than EPA or DHA [Mardones, 2008]; I recalculated the numbers after removing that study and still found a statistically significant impact (RR 0.89, 95% CI 0.80-0.99; Number Needed to Treat (NNT) 66, 95% CI 34-688; determined using an online calculator).
We’ll forcus on Cochrane’s finding for preterm birth < 34 weeks because it was stronger (2.7% vs. 4.6%; RR 0.58, 95% CI 0.44-0.77; 9 RCTs, 5204 participants) and the consequences are potentially more harmful.
There are three reasons why thee Cochrane report found a stronger benefit for DHA on preterm births than did the AHRQ report:
The data on omega-3s reducing the risk of preterm births < 34 weeks is stronger than data reducing the risk of preterm births < 37 weeks, but the AHRQ report only analyzed the latter.
The Cochrane analysis included one study, [Mardones, 2008] that used ALA, rather than DHA, which had a strong finding in reducing the risk of early preterm births (RR 0.19, 95% CI 0.04-0.88) whereas the AHRQ analysis didn’t include studies using ALA.
The AHRQ report separated their analysis into studies of DHA only (OR 0.87, 95% CI 0.66-1.15) and studies of DHA plus EPA (OR 0.86, 95% CI 0.65-1.15); dividing the findings into two groups likely weakened the statistical significance.
The Cochrane report also included three studies of women with diabetes [Horvaticek, 2017] [Min, 2014] and [Min, 2016], a study of women with a history of preterm birth [Bulstra-Ramakers, 1994], and women at high risk for pregnancy complications [Olsen, 2000].
I compiled the studies used by the Cochrane report in the spreadsheet, Preterm Delivery. After removing these five studies and the study using ALA, a benefit for DHA in preventing preterm delivery < 34 weeks remained (RR 0.49, 95% CI 0.24-0.71); the number needed to treat (NNT) is 60 (95% CI 38-150). I also calculated the statistics for the two studies that only included apparently healthy participants and for which gestational length was one of the primary outcomes: RR 0.24, 95% CI 0.09-0.67; NNT 25, 95% CI 15-72 [Carlson, 2013] [Harris, 2015].
Based on these studies, it appears that DHA supplementation can help prevent preterm births before 34 weeks. Could ALA also prevent them?
ALA Intake and Preterm Births
[Mardones et al. (2008, Chile)] provided low-income, pregnant women with a micronutrient-fortified milk powder. The women in the treatment group also were given ALA and LA. Using an intention-to-treat analysis (the analysis used by the Cochrane report), the treatment group had a lower risk of delivery before 34 weeks (RR 0.19, 95% CI 0.04-0.88; NNT 59, 95% CI 32-334). However, if you use the on-treatment analysis (women who followed the protocol more closely), the finding for ALA is weaker due to fewer preterm births in the placebo group (RR 0.23, 95% CI 0.05-1.07; NNT 54, 95% CI 28-1,117). It’s also possible that vitamin B6 could be a factor as the placebo group averaged below the DRI (1.64 ± 0.66 mg) while the treatment had a 30% higher intake (2.14 ± 1.21) which is above the DRI of 1.9 mg for vitamin B6 during pregnancy.
[Knudsen et al. (Denmark, 2006)] conducted a randomized, controlled study of fish oil or flax oil supplementation among over 3,000 pregnant women with low fish intakes. The treatment groups consisted of daily supplements of 100 mg EPA plus DHA, 300 mg EPA plus DHA, 700 mg EPA plus DHA, 1,400 mg EPA plus DHA, 2,800 mg EPA plus DHA, and 2,600 mg ALA. Supplementation didn’t start until an average of 22 weeks of pregnancy and continued until delivery. No differences in the length of gestation were detected between the fish oil or flax oil groups compared with a control group that received no intervention. When the results were limited to women with a usual dietary intake of < 150 mg per day of EPA plus DHA, there was no indication that omega-3 supplementation increased the length of gestation based either on an intention-to-treat or an on-treatment analysis. The length of gestation in a control group of women eating < 150 mg of EPA plus DHA per day was 40 weeks, suggesting that this population was not at risk for preterm births despite their low long-chain omega-3 intakes.
[de Groot et al. (2004)] conducted a double-blind, randomized, controlled intervention trial from week 14 of pregnancy until delivery. The subjects’ baseline daily ALA intake (at 14 weeks of pregnancy) was 1.3 g. The treatment group received 2.8 g of ALA plus 9.0 g of LA daily compared to only 10.9 g/day of LA for the control group. The control group’s ALA intake was measured again at week 36 and was 1.0 g/day. The treatment group had an average gestation length of 4.5 days longer than the controls which wasn’t statistically significant (P = .091). The incidence of preterm births wasn’t measured.
More research is needed to determine whether meeting the DRIs for ALA or increasing ALA intake beyond the DRIs, is as effective as DHA in preventing preterm births.
Timing of Intervention on Early (< 34 weeks) Preterm Births
Some of the studies on DHA supplementation and preterm births started the intervention rather late in pregnancy. Our spreadsheet, Preterm Delivery, lists the timing of the interventions with no clear pattern between the timing and a beneficial finding.
Of the three studies using ALA, one started the intervention at 11 weeks and found a statistically significant result [Mardones, 2008], one started at 14 weeks and found a non-significant trend [de Groot, 2004], and one started at 22 weeks with no positive impact [Knudsen, 2006]. This might be coincidental.
Official Recommendations
As of November 2022, the United States and Canada Dietary Reference Intakes don’t specifically recommend a DHA supplement during pregnancy or lactation.
There are other organizations that recommend DHA during pregnancy and nursing. Here I review the evidence used by the International Society for the Study of Fatty Acids and Lipids (ISSFAL) in some detail and also include the recommendations from the American Academy of Pediatrics.
ISSFAL Omega-3 Recommendations During Pregnancy and Nursing
In 2007, many organizations, including the International Society for the Study of Fatty Acids and Lipids (ISSFAL) published a Consensus Statement that recommends DHA intake of an average of at least 200 mg per day during pregnancy and nursing. They used two lines of reasoning.
The first line of reasoning is that the conversion of ALA to DHA is limited:
“The fractional conversion of a-linolenic acid to n-3 LC-PUFA may be greater in women than in men, which may contribute to meeting the demands of the fetus and the breastfed neonate for DHA, but most evidence indicates that the overall contribution of a-linolenic acid to DHA is limited; therefore, adequate intakes of preformed n-3 LC-PUFA, and in particular DHA, appear important for maintaining optimal tissue function (5-7).”
For this claim, citation 5 was a review paper by [JT Brenna (2022)] who is actually one of the authors of the Consensus Statement. However, I didn’t find Brenna’s review paper to provide evidence in favor of the statement’s claim. On the contrary, Brenna says:
“Failure to elevate 22:6n-3 [DHA] blood-compartment concentrations by 18:3n-3 [ALA] supplementation does not necessarily mean that 22:6n-3 concentrations do not increase in tissues. Conversion and conservation of 18:3n-3 may be efficient in developing neural tissue and in very active tissues such as retina which actively recycles 22:6n-3.”
Reliable measurements of these processes, however, are not possible without access to tissue samples and therefore are not possible for most tissues in humans. Animal studies of conversion efficiency are of limited value because of physiological differences, as cited below.
Citation 6 was a paper by [GC Burdge (2005)] which says:
“Overall, [ALA] appears to be a limited source of longer chain n-3 PUFA in humans. Thus, adequate intakes of preformed long chain n-3 PUFA, in particular DHA, may be important for maintaining optimal tissue function.”
However, as reviewed in this article’s appendix, Evolutionary Arguments for a Dietary Requirement for DHA, Burdge subsequently published a paper in 2022 in which he argues that ALA is an adequate source for meeting the omega-3 needs of infants” [Burdge, 2022].
Citation 7, a review by [SM Innis (2005)], provides an analysis of DHA amounts in the brain and argues that preterm infants cannot produce enough DHA to supply the brain with this amount. But the review seems to suggest that, at most, we don’t know whether term infants can benefit from DHA supplementation.
The Consensus Statement’s second line of reasoning is based on the clinical trials of DHA supplementation during pregnancy and nursing which the authors believed showed beneficial effects on infant development. They cite eight clinical trials, all of which are included in the 2016 report from the Agency for Healthcare Research and Quality reviewed above [Newberry, 2016]. We discuss this and subsequent clinical trials in detail above.
American Academy of Pediatrics DHA Recommendations during Nursing
In their Technical Report: Breastfeeding and the Use of Human Milk, the American Academy of Pediatrics (AAP) says, “The mother’s diet should include an average daily intake of 200 to 300 mg of the omega-3 long-chain polyunsaturated fatty acids for adequate preformed docosahexaenoic acid DHA in the mother’s milk and to improve the infant’s fatty acid status [Meek and Noble, 2022].”
The AAP doesn’t provide a rationale for their recomendation in this Technical Report, but the rationale they provide in their 2019 edition of Pediatric Nutrition doesn’t include anything important that wasn’t covered here. The AAP doesn’t provide recommendations for pregnancy.
Omega-3s and Chronic Disease
Most of the concern with regard to low plasma levels of EPA and DHA among vegetarians is due to studies that have found an association between low EPA and DHA blood levels and an increased risk of chronic diseases such as cardiovascular, cognitive decline, and depression.
These associations have generally been consistent but weak. There have also been some associations between omega-3 blood levels and an increase in some chronic diseases. In this section we review the evidence.
Omega-3s and Cardiovascular Disease
Research on omega-3s and cardiovascular disease has examined the associations with fish consumption, blood levels of omega-3s, and omega-3 supplementation.
Fish Consumption and Cardiovascular Disease
As of February 2021, the American Heart Association was still basing its omega-3 fatty acid recommendations on its 2002 position paper, Fish consumption, fish oil, omega-3 fatty acids, and cardiovascular disease [Kris-Etherton, 2002] which recommends that adults “Eat a variety of (preferably oily) fish at least twice a week. Include oils and foods rich in alpha-linolenic acid (flaxseed, canola, and soybean oils; flaxseed and walnuts).”
Some recent reports include:
A 2020 meta-analysis of six cohort studies found no correlation between eating fish and a reduced risk of cardiovascular disease or mortality [Zhong, 2020].
A 2020 Cochrane review determined that there wasn’t enough evidence to assess the impact of eating fish on cardiovascular health [Abdelhamid, 2020].
A 2016 meta-analysis of 12 prospective studies found a reduced risk of mortality with increasing fish intake [Zhao, 2016].
Omega-3 Supplementation and Cardiovascular Disease
In what they called “the most extensive systematic assessment of effects of omega-3 fats on cardiovascular health to date,” a 2020 Cochrane Review analyzed 86 randomized controlled trials of 12 to 88 months duration using omega-3 capsules, omega-3-enriched food, or dietary advice to eat more omega-3s [Abdelhamid, 2020].
The review found little to no effect of increasing omega-3s on all-cause or cardiovascular mortality, cardiovascular events, stroke, or arrhythmias. Increased omega-3 intake showed a trend with reduced coronary heart disease mortality (RR 0.90, CI 0.81-1.00) and there was a reduced rate of coronary heart disease events (RR 0.91, CI 0.85-0.97).
Increasing long-chain omega-3s reduced triglycerides by ~15% in a dose‐dependent way. Overall, the authors stated that 334 people would need to increase their long-chain omega-3 intake to prevent one person from having a coronary heart disease event and they believed this wasn’t enough of an impact to recommend supplementation.
In contrast, a 2019 meta-analysis of omega-3 supplementation found a benefit from omega-3 supplementation in the combined results from 13 randomized controlled trials using about 800 to 1,800 mg of omega-3 fatty acids per day [Hu et al.].
At baseline, the participants had a mixed risk for cardiovascular disease: 40% had diabetes and 73% were using cholesterol-lowering medication. In one set of results, that excluded the REDUCE-IT trial described below, they found a reduced risk of heart attack (RR 0.92, CI 0.86-0.99) and cardiovascular death (RR 0.93, CI 0.88-0.99).
The omega-3 supplementation in this set of results is arguably higher than the AHA recommendations of at least 2 servings of fish per week, but not implausible. For the omega-3 content of fish, see Omega-3 Fatty Acids: Fact Sheet for Health Professionals.
The Reduction of Cardiovascular Events with Icosapent Ethyl-Intervention Trial (REDUCE-IT) was excluded from Hu et al.’s results above because it used a much higher dose of omega-3s: 4,000 mg/day of a purified form of EPA. It showed markedly better success for heart attack (RR 0.69, CI 0.58-0.81) and cardiovascular death (RR 0.80, CI 0.66-0.98).
Participants also had a lower risk of stroke (RR .72, CI 0.55-0.93), but their death from all causes wasn’t significantly lower (RR .87, CI 0.74-1.02) than the placebo [Bhatt, 2019]. The extremely high amount of EPA used in REDUCE-IT is a pharmacological dose and not relevant to dietary omega-3 intake.
Stroke and Omega-6 to Omega-3 Ratio
[Cupino et al. (2022)] analyzed the ratio of omega-6 to omega-3 intakes and risk of stroke among the Adventist Health Study-2 cohort. They found a statistically significant association between omega-6 to omega-3 ratio and an increased risk of any type of fatal stroke (HR 1.40, 95% CI: 1.16-1.69) for the 90th percentile ratio (12:1) vs. 10th percentile ratios (6:1).
Omega-3s and Cognition
A 2012 cross-sectional report from the Framingham Study examined 1,575 people (54% women) with an average age of 67 (SD 9) years with respect to omega-3 blood levels and numerous cognitive-related parameters [Tan, 2012].
They compared the EPA+DHA red blood cell membrane fatty acids in the lowest quartile (≤4.4%) to those in the upper three quartiles (75th percentile was 6.5%). They found that those in the lowest quartile had a significantly lower cerebral brain volume (equivalent to approximately two years of brain aging), but a similar white matter hyperintensity volume, temporal horn volume, and rate of silent stroke. Low blood EPA+DHA was associated with a poorer score on some tests of cognition.
As part of the Women’s Health Initiative Study of Cognitive Aging, [Ammann et al. (2013, USA)] conducted a cross-sectional analysis of 2,302 women 65 years and older and found no difference in cognition between those in the upper one-third compared to those in the lowest one-third of EPA+DHA percentage of fatty acids in red blood cells. However, the lowest one-third had an average EPA-plus-DHA of 3.8% which is quite a bit higher than vegans tend to have, so this finding doesn’t necessarily reassure us about the omega-3 status of vegans. A 2017 study by Ammann et al. (described below), followed a much larger group of participants over time and provides more insight into whether higher EPA and DHA percentages are important in preventing cognitive impairment and dementia, especially in older women.
[Zhang et al. (2016)] conducted a meta-analysis of 21 case-control and prospective studies and found that increases of 1-serving/wk increments of fish were associated with a reduced risk of dementia (RR 0.95, CI 0.90-0.99) and Alzheimer’s disease (RR 0.93, CI: 0.90-0.95). DHA intake was also inversely associated with risks of dementia (RR 0.86, CI 0.76-0.96) and Alzheimer’s disease (RR 0.63, CI 0.51-0.76).
However, blood levels of omega-3 fatty acids were not associated with a reduced risk of these or other cognitive diseases. In a letter to the editor, Koch and Jensen point out that in the six studies looking at the association between fish intake and dementia and Alzheimer’s disease, one study was a 2-year follow-up of another study with a longer follow-up.
[Koch and Jensen] argue that “Appropriate exclusion of the report from Kalmijn et al. would render the meta-analysis of fish intake in relation to dementia risk insignificant (RR: 0.96; 95% CI: 0.91, 1.01; no heterogeneity) and change the RR estimate for AD risk to 0.87 (95% CI: 0.77, 0.98) in a random-effects meta-analysis with significant between-study heterogeneity still present.”
[Zhang and Jiao] responded that it was appropriate to include both reports. It’s perplexing that omega-3 intakes but not blood levels would be associated with a reduced risk of dementia if there is a true effect, though it might suggest that blood levels of EPA and DHA aren’t an accurate representation of omega-3 status.
[Amman et al. (2017, USA)] conducted the largest prospective study to assess the risk of dementia with omega-3 fatty acid status. The study was part of the Women’s Health Initiative Memory Study testing the impact of the hormones estrogen and progestin on the memory of women ≥65 years old. Although the hormone part of the study was concluded early, the researchers continued to follow 6,706 women for an average of 9.8 years to see if baseline EPA and DHA levels were associated with a diagnosis of probable dementia (PD) or mild cognitive impairment (MCI).
The study compared the risk of PD and MCI among those with EPA/DHA within one standard deviation above the mean (5.3-6.8% EPA+DHA) to those within one standard deviation below the mean (3.8-5.3% EPA+DHA). In one of their models, the researchers found a statistically significant reduction in PD (HR 0.91, CI .83-.99), but most models found no significant association including one that adjusted for the APOE genotype associated with Alzheimer’s Disease (HR 0.92, CI 0.83-1.01).
The researchers calculated that the increased risk of PD represented a 2% reduced risk (12% vs. 14%) of PD incidence over a 15-year period. There were no significant associations between EPA+DHA and MCI. Examining EPA and DHA separately produced no significant findings.
In summary, studies of omega-3 fatty acids conducted on populations of omnivores consistently find some significant associations with better cognition, though they tend to be weak. That dietary intakes are more strongly associated with better cognition, than are blood levels, raises a question about whether omega-3s are responsible for the beneficial association rather than other variables paired with omega-3 intake.
Omega-3s and Depression
Our interest in omega-3s and depression is mostly related to whether vegetarians are at an increased risk of depression due to lower EPA or DHA levels.
Risk of Depression
[Deane et al. (2019)] conducted a meta-analysis and systematic review of 32 randomized controlled trials and found no effect of increasing EPA and DHA on the risk of depressive symptoms (RR 1.01, CI 0.92-1.10). Studies had a median duration of 12 months with a median dose of 0.95 grams per day (ranging from 0.4 to 3.4 grams per day). One study addressed omega-3s and anxiety and found little to no effect. The researchers recommend against taking omega-3 supplements for reducing depression and anxiety risk.
Treatment for Depression
Whether EPA or DHA can be used to treat people with depression is only loosely related to the omega-3 status of vegetarians, but it’s where most of the research has focused and so we review it here.
Early research on treating depressive symptoms with supplementation of EPA and DHA was mixed. In a 2006 review, [Sontrop and Campbell] found that supplementation improved depression but it wasn’t clear whether it was effective for depressed patients in general or only those with abnormally low concentrations of EPA and DHA.
In another 2006 review, [Appleton et al.] found “little support” based on the small number of trials with significant variation. In a 2007 meta-analysis [Lin and Sue] found a positive effect of supplementation but with significant publication bias. In a 2009 meta-analysis, [Martins] found evidence that EPA is more effective than DHA.
[Grosso et al. (2014)] conducted a meta-analysis of 11 trials of patients with a DSM-defined diagnosis of a major depressive disorder (MDD) and 8 trials of patients with depressive symptomatology but no diagnosis. They found supplementation to have a beneficial effect for the patients diagnosed with MDD and also for those with bipolar disorder. They considered EPA to be more effective, with many trials using pharmacological doses. [Hallahan, et al. (2016)] found similar results in their meta-analysis.
In their meta-analysis, [Luo et al. (2020)] found a benefit from high-dose (≥2 g/day) but not low-dose (<2 g/day), EPA/DHA supplementation in the early therapy period for MDD.
Omega-3s and Increased Risk of Disease
Some studies have associated higher omega-3 intakes with an increased risk of disease.
Prostate Cancer
A meta-analysis of randomized controlled trials [Hanson, 2020] measured the impact on the risk of a prostate cancer diagnosis of a higher long-chain omega-3 intake (7 trials, RR 1.10, 95% CI 0.97-1.24, NNTH 334) and of a higher ALA intake (2 trials, RR1.30, 95% CI 0.72–2.32, NNTH 334). Neither finding was statistically significant and had a high number needed to harm (NNTH). There was no impact on overal cancer diagnosis or death. The authors provided a chart showing that the benefits of higher omega-3 intake on cardiovascular events outweighed the potential harm.
A meta-analysis [Carleton, 2013] of case-control and prospective studies found no association between ALA intake and prostate cancer (RR 1.08, 95% CI 0.90-1.29). Removing one study during sensitivity analysis resulted in a weak, non-significant protective effect of ALA (RR 0.91, 95% CI 0.83-0.99, p=0.02).
A systematic review and meta-analysis [Simon, 2009] of ALA blood or tissue concentrations and prostate cancer found no association after adjustment for publication bias (RR: 0.96, 95% CI 0.79-1.17).
A 2010 meta-analysis found that subjects who consumed more than 1.5 g/day of ALA had a significantly decreased risk of prostate cancer (0.95, 0.91-0.99) compared to those who ate less [Carayol, 2010].
A 2018 paper from Harvard School of Public Health suggested that past associations between ALA and prostate cancer might have been due to trans-ALA which has been largely removed from the food supply [Wu, 2018].
A case-control study from the SELECT trial [Brasky, 2013] found an association between higher DHA phospholipid levels and prostate cancer. This finding is superceded by the findings of Hanson et al. (2020) described above, but a discussion of this finding from 2013 can be found on the JackNorrisRD.com blog post, DHA Supplements and Prostate Cancer. [[blog]]
Eyesight
A 2001 analysis from the Nurses Health Study found an almost statistically significant increase in age-related macular degeneration for those with the highest ALA intake [Cho, 2001, USA].
In contrast, a 2013 study found that higher ALA levels in the blood were associated with a lower risk of late age-related macular degeneration [Merle, 2013, France]. And a 2017 follow-up from the Nurses Health Study found that a high intake of ALA was associated with an increased risk of intermediate age-related macular degeneration before 2002, but not afterward when less trans fats were found in participants’ blood [Wu, 2017, USA].
A 2005 analysis from the Nurses Health Study found that both the highest intakes of ALA and LA were associated with an increase in lens opacity, which can lead to cataracts [Lu, 2005, USA]. For ALA, the risk ratio was 2.2 (1.2, 4.5) for about 1.26 g compared to .86 g per day. A 2007 analysis of the same group found that the highest category of ALA intake (about 1.26 g per day) was linked to a 16% increase in eye lens nuclear density compared to the lowest category (about .84 g per day) over five years. As of 2018, no follow-up studies appear to have been conducted on ALA and cataracts [Lu, 2007, USA].
Without more definitive research we don’t believe concerns about eyesight is any reason to avoid plant-based ALA due to the small differences in ALA intake in these studies, the fact that much ALA in meat-based diets comes from animal products, that trans ALA is no longer added to the food supply, and the large number and inconsistencies of associations between different fatty acids and various conditions.
Appendix A: Biomarkers of DHA Status
The primary reason why researchers rely on plasma and/or red blood cell percentages is convenience: they’re the most accessible and straightforward measurements to obtain. Studies consistently find inverse associations, albeit weak, between blood percentages and morbidity which bolsters their use.
In their review, Biomarkers of DHA status, [Kuratko and Salem (2009)] argue that the percentage of fatty acids as DHA in plasma or red blood cells is a generally adequate marker of overall DHA status. However, they also highlight many of the caveats that we discuss in Conversion of ALA to EPA and DHA.
Kuratko and Salem cite one paper worth discussing here. In a gruesome experiment, [Sarkadi-Nagy et al. (2004)] studied baboon infants in order to measure various fatty acids in their blood and tissues. At 14 days old, the infants were given a carbon-tracer labeled dose of ALA. After another 14 days, they were killed and the researchers measured correlations between the carbon-labeled DHA in plasma and red blood cells with carbon-labeled DHA in the brain, retina, and liver. R-coefficients are listed in the table below.
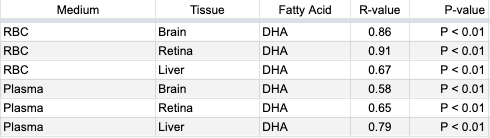
Kuratko and Salem summarize Sarkadi-Nagy et al.’s results by saying, “Both erythrocyte and plasma levels were correlated with resulting DHA content in brain, retina, and liver.” But these correlations weren’t between the total percentage of fatty acids as DHA; rather they were the percentage of fatty acids as DHA that was converted from ALA during the study period.
In contrast, in their Table 3, Sarkadi-Nagy et al. list the total amounts of various fatty acids in plasma, red blood cells, and tissues and while there were some similarities there were also many differences.
Sarkadi-Nagy et al. write, “It is widely recognized that tissue and plasma [fatty acid] concentrations respond to diet. Improvements in function cannot be directly inferred and must be demonstrated (43). Furthermore, the wide variation in the regulation of individual [fatty acid] concentrations from tissue to tissue makes extrapolation difficult from compartments accessible in humans, primarily plasma and RBCs.” In other words, for their view that blood levels of DHA are adequate markers of omega-3 status, Kuratko and Salem rely on a paper by Sarkadi-Nagy et al. who disagree that tissue status can be extrapolated from blood percentages.
Kuratko and Salem also cite research on rhesus monkeys and then summarize by stating, “Although a statistical correlation was not reported, it is evident that a positive relationship exists between erythrocyte DHA levels and tissue levels, including the brain cortex and retina [68,69].” Their citation 68, [Pawlosky et al. (1997)], didn’t measure fatty acid levels in erythrocytes. Their citation 69, [Pawlosky et al. (2001(a))], used a carbon tracer to measure the conversion of ALA to EPA and DHA in human blood but not tissues.
Kuratko and Salem’s paper also includes a citation 58, [Pawlosky et al. (2001(b))], which refers to the research using rhesus monkeys, but the paper wasn’t readily available and the abstract doesn’t indicate that the study would support their claim.
At the time of their writing, Kuratko and Salem were employees of Martek Biosciences which could arguably benefit from a convenient biomarker of DHA status that would err on the side of overestimating the need for DHA supplementation.
There are likely many other studies not mentioned in this article that have drawn various comparisons between percentages of long-chain omega-3 fatty acids in blood and tissues. The correlations do exist in some populations, but they are vague and cannot be used to draw any definite conclusions about the omega-3 status of apparently healthy individuals.
Appendix B: Evolutionary Arguments for a Dietary Requirement for DHA
A nutrient is essential if it must be provided by the diet for optimal health. A nutrient is conditionally essential if it’s required in the diet only under suboptimal conditions.
There’s an evolutionary argument that DHA is an essential nutrient, which goes:
“For long periods of our evolution, humans lived near large bodies of water that provided a plentiful source of dietary DHA through fish. This plentiful DHA allowed the human brain to grow in size and intelligence. As a result, humans are still dependent on a source of dietary DHA for optimal brain health.”
Short-chain omega-3 and omega-6 fats compete for the same enzymes to be elongated. Due to this, there’s also an evolutionary argument that DHA is a conditionally essential nutrient:
“In modern diets, people eat such large amounts of omega-6 fats that the body’s ability to produce enough DHA to compete against the omega-6s is compromised. Under the suboptimal condition of a high omega-6 intake, dietary DHA becomes essential.”
My focus is primarily on the first evolutionary argument—whether humans require a dietary source of DHA due to an evolutionary dependence on eating fish. However, the research I will review sometimes conflates the two arguments and so I wanted to describe them both at the outset.
There are four life stages when DHA could be either essential or conditionally essential:
During fetal development, the fetus is at least partially dependent on obtaining DHA from the mother.
Infants might be dependent on a dietary source of DHA from the mother’s breast milk or formula.
During pregnancy or lactation, without a dietary source of DHA, the mother might not be able to convert enough ALA into DHA to provide for herself and her infant’s needs.
During adulthood, a dietary source of DHA may be required to prevent cognitive decline.
Whether infants require a dietary source of DHA for optimal brain development isn’t relevant to the argument that humans have evolved with a dependence on eating fish because infants can obtain dietary DHA from breastmilk, and so I don’t spend much time addressing this question.
I also don’t address arguments about the food sources of pre-modern humans because even if pre-modern humans ate ample amounts of fish, it wouldn’t mean that modern humans have a dietary requirement for DHA.
Instead, I review the evidence for what I consider to be the most persuasive arguments for dietary DHA being essential. Some of these arguments are ecological, such as claims that human brain size and intelligence have decreased while neurological issues and mental illness have increased due to a move away from an aquatic diet. I also address specific physiological claims about the metabolism of omega-3s based on clinical research. Much of this research used animals.
Below, I review three published papers arguing that humans evolved on an aquatic diet that included fish and, therefore, included a consistent, dietary source of DHA that increased our brain size and intelligence. They imply that we still depend on dietary DHA for optimal brain development and maintenance. I also review two papers arguing that there’s no dietary need for DHA beyond infancy.
Crawford, 2006 and Crawford et al., 2022
Michael A. Crawford is a researcher with the Institute of Brain Chemistry and Human Nutrition in the U.K. He’s published scientific papers, sometimes with co-authors, arguing that omega-3s are neglected nutrients in the modern world and that a dietary source of DHA was important for the evolution of the human brain and is still important for infant brain development.
I’ll address what I consider to be the most persuasive arguments in his articles, [Docosahexaenoic acid in neural signaling systems (2006)] and [Neurodevelopment, nutrition and genetics (2022)].
Crawford’s 2006 article appears to be a response to [John Langdon’s 2006] paper arguing that there’s no evolutionary requirement for DHA beyond infancy, which I review later (below). Crawford says that “[Langdon] neglects the basic principle of Darwinian evolution. The well documented greater efficiency of preformed docosahexaenoic acid for brain incorporation during development would have conferred a distinct survival advantage over those without it.”
But despite his many arguments and citations, Crawford provides little more than conjecture that a dietary source of DHA, beyond what is in breastmilk, is required for the proper development of the human brain. Instead, he cites evidence that omega-3s, which could be in the form of ALA, are required.
For example, [Crawford (2006)] writes that “DHA in the diet is rapidly and selectively incorporated in brain cell membranes and is concentrated at synaptic signaling sites [Suzuki et al., 1997].” In this study by Suzuki et al., male mice were deprived of omega-3s for 11 days and then placed in a diet group for either 6 or 30 days. There were numerous groups of mice, but I’ll limit this summary to the dietary groups of no omega-3s, ALA, and DHA. The table below shows the levels of DHA among the various groups of mice at the end of each trial.
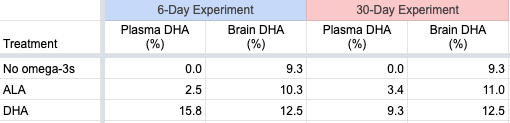
The plasma levels vary considerably, while the brain levels are similar. The physiological significance of the differences in the brain percentages of DHA between the ALA and DHA-fed groups wasn’t determined.
Arguably, this study provides reassurance that, at least for mice, ALA as the only dietary source of omega-3s may be adequate. But since mice in the wild are unlikely to have evolved with a significant source of dietary DHA, these results can’t necessarily be applied to humans.
Crawford (2006) writes:
“Deficiency studies in rodents (Sinclair and Crawford, 1973), primates (Fiennes et al., 1973, Neuringer et al., 1976) and visual and cognitive trials in human infants (Birch et al., 2000) have indicated that DHA is essential to brain development and function.”
[Sinclair and Crawford (1973)] don’t isolate DHA in any way to justify this claim. [Fiennes et al. (1973)] studied omega-3 deficiency, not DHA deficiency. [Neuringer et al. (1986)] studied diets low in ALA. [Birch et al. (2000)] showed that infants who weren’t breastfed, but who had DHA in their infant formula, performed better on some cognitive and motor skills tests than infants without DHA in their infant formula.
On an epidemiologic level, Crawford argues that a move away from aquatic diets has caused a deficiency of important nutrients, most notably DHA and iodine, that has led to a global increase in mental disorders, and a reduction in intelligence and brain size. I’ll address these points but, because these topics are vast, I’m merely doing a cursory review.
Mental Health and Brain Disorders
Crawford (2006) writes:
“The rise in mental ill health and brain disorders, to replace all other costs in the European list of burdens of ill health, raises interesting questions as to its association with the reduced availability and consumption of marine and fresh water products.
In 1972, based on the changing diet and lipid science, we predicted brain disorders would rise and this has now happened. Brain disorders now account for the highest cost to the burden of ill health in the EU (€386 billion) having overtaken heart disease, cancer and obesity by a large margin. This is hardly surprising. The brain first evolved in the sea and still uses marine fatty acids; the loss of the marine food chain is bound to have consequences.”
In 2022, Crawford et al. continued to emphasize this argument saying, “One in five adults in US are reported to live with mental illness in 2019, prior to the pandemic [National Institutes of Health]; the number of 197.3 million in India suffer from mental disorders in 2017 is of the same order, double digit percentage of population [GBD India].”
Is Crawford correct that brain and mental illnesses are increasing?
According to the paper, [Global, regional, and national burden of neurological disorders, 1990–2016], the absolute numbers of neurological disorders are increasing due to an aging population, but after adjusting for age and other variables, the rates are actually decreasing. For this analysis, they included a wide range of diseases, some that seem unlikely to be related to a DHA deficiency. Here’s a list of some specific diseases and the percentage of increase (+) or decrease (-) in their age-adjusted incidence between 1990 and 2016: stroke (-8%), Alzheimer’s disease and other dementias (+2%), Parkinson’s disease (+22%), idiopathic epilepsy (+6%), multiple sclerosis (+10%), and migraine (-2%).
Regarding mental illness, Crawford et al. (2022) cite the National Institutes of Health web page, Mental Illness. While the page doesn’t assess whether mental illness is increasing, they say that any mental illness (AMI) affects a large percentage of U.S. adults (21% as of 2020). AMI is defined as a mental, behavioral, or emotional disorder and can vary in impairment, ranging from none to mild, moderate, or severe.
Regarding severe mental illness, the prevalence was 5.6% of all U.S. adults, with it being higher among adults aged 18-25 (9.7%) than adults aged 26-49 (6.9%) and aged 50+ (3.4%). Based on data from the National Comorbidity Survey Adolescent Supplement, 49.5% of adolescents had AMI; of those, 22.2% had severe impairment.
Regarding mental illness in India, Crawford et al. (2022) cite [The burden of mental disorders across the states of India: the Global Burden of Disease Study 1990-2017] which found that the contribution of mental disorders to the total disability-adjusted life-years (DALYs) in India increased from 2.5% in 1990 to 4.7% in 2017. In 2017, depressive disorders contributed the most to the total DALYs (33.8%), followed by anxiety disorders (19.0%), idiopathic developmental intellectual disability (10.8%), schizophrenia (9.8%), bipolar disorder (6.9%), conduct disorder (5.9%), autism spectrum disorders (3.2%), eating disorders (2.2%), and attention-deficit hyperactivity disorder (0.3%). Dementia wasn’t mentioned in this report.
These rates of mental illness do seem rather high but some suggest it’s due to higher reporting. An article in The Guardian, Mental illness: is there really a global epidemic? (June 3, 2019) reports that in the previous 20 years, two variables have impacted the rates of mental illness: recognition and destigmatization. This has resulted in more people seeking help and reporting mental distress. Harvey Whiteford, professor of population mental health at the University of Queensland is quoted as saying, “All the modelling we’ve done in high-income countries where there’s survey data which has tracked over time shows that the prevalence hasn’t changed–it’s flatlined.”
The idea that brain disorders and mental illnesses are increasing due to a lack of dietary DHA is an interesting hypothesis which, at best, is difficult to assess.
Intelligence
Crawford et al. (2022) argue that worldwide average intelligence quotients (IQ) peaked in the birth year 1975 and then fell steadily through the birth year 1990. While Figure 1 in their paper shows a consistent trend, the difference is only about 2.5% of a normal IQ.
Norway is an interesting case regarding the decrease in IQ compared to per capita fish consumption. An article from the World Economic Forum, IQs are falling – and have been for years (2018), provides data from Norway where men reporting for national service between 1970 and 2009 were given IQ tests.
It says “[The] analysis showed that the men born in 1962 had higher scores than those born in 1991. Those born in 1991 scored five points lower than those born in 1975, and three points lower than those born in 1962. This is the opposite of what happened during much of the 20th century when IQ scores rose by around 3% a year.”
Norway has one of the highest per-capita fish intakes of any country. The HelgiLibrary created a graph using FAOSTAT data, Fish Consumption Per Capita in Norway, showing an increase from about 41 kg in 1960 to about 53 kg in 2013. The increase in per-capita fish consumption in Norway during the time that IQ was decreasing suggests that the decrease in IQ was not due to a drop in fish consumption.
Norway was the only country for which I found data accessible enough to make this comparison. Based on this data from Norway, it seems unlikely that decreases in intelligence are due to a move away from an aquatic-based diet.
Brain Size
Crawford et al. (2022) write:
Dr Marta Lahr from the UK Cambridge University’s Leverhulme centre for Human Evolutionary Studies presented her findings to the Royal Society in 2013 that the brain size of the modern-day humans has been shrinking since the beginning of the land-based agriculture and animal husbandry 10,000 years ago.
For this statement, Crawford et al. cite a short news article, Farming to blame for our shrinking size and brains (by Deborah Braconnier, Phys.org, 2011).
This article ends with:
“Agriculture however does not explain the reduction in brain size. Lahr believes that this may be a result of the energy required to maintain larger brains…This reduction in brain size however does not mean that modern humans are less intelligent. Human brains have evolved to work more efficiently and utilize less energy.”
A related article, Are brains shrinking to make us smarter? (by Jean-Louis Santini, Phys.org, 2011) says:
“But the downsizing does not mean modern humans are dumber than their ancestors — rather, they simply developed different, more sophisticated forms of intelligence, said Brian Hare, an assistant professor of anthropology at Duke University.”
A 2019 article from Discover, The Human Brain Has been Getting Smaller Since the Stone Age (by Bridget Alex), says that the most likely explanation for a reduction in human brain size is the survival of the friendliest:
“The idea is, within Stone Age societies, cooperative, level-headed individuals were more likely to survive and reproduce than combative, aggressive ones. Those pro- or anti-social inclinations were influenced by genes regulating hormones, which also affected physical traits, including body and brain size. Over time, “survival of the friendliest” led to humans with slighter builds and brains on average. So although there was a reduction in skull size—and possibly intelligence—human cooperation grew, cultivating greater collective wisdom.”
I don’t consider these news articles to be scientifically rigorous, but they suggest that a move away from an aquatic diet isn’t the accepted explanation for a reduction in brain size and that this reduction in brain size isn’t indicative of a health crisis.
Genetics and the n6:n3 Ratio
Crawford et al. (2022) propose a theory that traditional vegetarian societies, such as in the Pune region of India, tend to have genetic variants for fatty acid conversion that lead to low conversion of ALA to DHA when omega-6 intakes are high (such as in modern diets), regardless of how much ALA is added to the diet. If true, DHA would be conditionally essential in these contexts, but this is different from the claim that humans evolved with a dietary requirement for DHA due to a reliance on an aquatic-based diet.
Bradbury, 2011
In 2011, Dr. Joanne Bradbury from the School of Health and Human Sciences of Southern Cross University in Australia, published the paper, [Docosahexaenoic acid (DHA): an ancient nutrient for the modern human brain].
Bradbury argues that modern humans have adapted to a dietary intake of preformed DHA. Bradbury’s arguments are based on the idea that endogenous synthesis of DHA from ALA in humans is “much lower and more limited than previously assumed.” Bradbury attributes the supposedly limited conversion of ALA to DHA to an increase in omega-6 intake. She also cites research with infants suggesting that dietary DHA is critical for their development, which, as I point out above, is available through breastmilk and doesn’t provide evidence for an evolutionary need for eating fish.
Langdon, 2006
In 2006, John Langdon of the Departments of Biology and Anthropology at the University of Indianapolis wrote a paper, [Has an aquatic diet been necessary for hominin brain evolution and functional development?], arguing that an aquatic food supply was not critical for the evolution of the human brain nor is DHA essential for the brain development of children today.
Langdon reviews a wide range of topics. For example, he cites a survey finding that of 123 modern hunter-gatherer groups, fishing didn’t provide a measurable part of the diet in 23.
In my opinion, this excerpt sums up Langdon’s strongest argument:
“An overall body deficiency [of DHA] permits DHA to be substituted by other fatty acids within the membranes, including docosapentaenoic acid (22:5n-6) [omega-6 DPA] or arachidonic acid (20:4n-6) [AA], so that body tissue composition can shift fairly quickly as diet changes (Neuringer et al. 1988; Uauy, 1990; Neuringer, 1993). This replacement may be temporary, until body levels of DHA are restored, and it implies that temporary shortages of DHA need not interfere with the rate of overall brain growth.”
Let’s see what evidence Langdon cites to support this view.
I’m not sure why Langdon cites the [1993 paper by Neuringer]. In that brief review, Neuringer describes a study in which infants who had been fed formula without DHA had lower levels of DHA (7.0-7.5%) in their cerebral cortex compared to those who received breastmilk (~9.75%). This was despite the fact that one group of formula-fed infants was older (16-43 weeks) than the breastfed infants (5-16 weeks) and that DHA normally accumulates in the brain as infants age. This study didn’t address whether omega-6 DPA or AA could adequately replace DHA and, therefore, doesn’t support Langdon’s argument.
The 1988 review by [Neuringer et al.] seems more relevant. They say:
“As first observed by Mohrhauer & Holman, decreases in DHA were compensated by increases in the n-6 fatty acids 22:5n-6 and, to a lesser extent, 22:4n-6. Consequently, the total level of 22-carbon polyunsaturated fatty acids remained roughly constant, and the degree of polyunsaturation changed only slightly. This reciprocal replacement of DHA by long-chain n-6 fatty acids is a consistent finding in studies of n-3 fatty acid deficiency. It is particularly striking because, with a few exceptions, 22:5n-6 is normally present at very low levels in animal tissues. Therefore, the ratio of 22:5n-6 to 22:6n-3 in blood and tissues has been suggested as an index of n-3 fatty acid deficiency [Galli et al., 1974].”
Neuringer et al. strongly imply that replacing DHA with omega-6 DPA isn’t optimal. In examining their citations, the study by [Mohrhauer and Holman (1963)] used rats and didn’t assess any potential problems with substituting the long-chain omega-6 fatty acids for DHA. Similarly, the study by Galli et al. used rats and didn’t assess the impacts of substituting long-chain omega-6 fatty acids for DHA.
Finally, the [1990 review by Uauy] cited by Langdon doesn’t provide evidence to support Langdon’s statement. Uauy actually argues that infants require a dietary source of DHA.
While I’m sympathetic to much of what Langdon writes and would prefer that it be true, the most critical part of his paper doesn’t convince me.
Burdge, 2022
Graham Burdge is a lipid researcher from the University of Southampton in the U.K and was the lead researcher on a series of omega-3 conversion studies [Burdge et al., 2002] [Burdge and Wootton, 2002] [Burdge et al., 2003].
In 2022, Burdge published a paper, [α-linolenic acid interconversion is sufficient as a source of longer chain ω-3 polyunsaturated fatty acids in humans: An opinion]. In this thorough review article, Burdge argues that a dietary intake of ALA is sufficient to meet the body’s needs for EPA and DHA.
Rather than being concerned that vegetarians might need to supplement with DHA, Burdge argues that the apparently healthy status of long-term vegetarians and vegans suggests that there is no dietary need for EPA and DHA.
Burdge says that in an omega-3 deficiency, omega-6 DPA accumulates in the plasma phospholipids and that the few studies of vegetarians that have reported omega-6 DPA levels have not found an accumulation. Burdge points out that [Sanders and Reddy (1992)] found no accumulation of omega-6 DPA in the red blood cells of infants breastfed by vegan mothers.
However, Burdge doesn’t include that [Sanders and Reddy (1992)] also found higher amounts of omega-6 DPA for Hindu vegetarians compared to omnivores in cord plasma (2.34% vs. 1.58%) and artery phospholipids (4.15% vs. 3.19%). These fractions weren’t reported for vegans.
The Hindu vegetarians had ALA intakes of only 0.9 g/day compared to 1.2 g/day for the vegans. While this difference isn’t much, 0.9 g/day is lower than the recommended DRI for omega-3s of 1.1 to 1.4 g/day and might be low enough that these Hindu vegetarians were deficient in omega-3s.
Burdge writes:
“The findings of dietary supplementation trials and experiments using stable isotope tracers have been interpreted as indicating that humans are “poor” converters of [ALA], in particular with respect to DHA synthesis. The use of the terms “poor,” constrained or “limited”, [or] severely “restricted” to describe PUFA synthesis in humans presupposes that the level of conversion should be greater, but what this higher level should be has not been defined and is potentially misleading.
Rather, capacity for hepatic [ALA] conversion in humans is better considered as a product of an evolutionary history and, therefore, nutritionally adequate.”
Conclusion to Evolutionary Arguments for a Dietary Requirement for DHA
The evolutionary arguments in favor of a dietary requirement for DHA are interesting but the evidence seems too vague to know whether they’re true. It appears that whether modern humans require dietary DHA for proper brain development and maintenance is a question that can only be answered through clinical trials comparing outcomes in people with and without a dietary source of DHA.
Appendix C: Stereodonic Acid
Stearidonic acid is a shorter-chain omega-3 that is unique because it does not require the rate-limiting enzyme that ALA requires to convert to EPA. There are very few plant-based foods that naturally contain SDA, specifically the oils of Echium plantagineum (echium) and Buglossoides arvensis (Ahiflower). There also are genetically modified soy and canola oils that are enriched with SDA.
Last updated December 2022
Bibliography
___Agren JJ, Törmälä ML, Nenonen MT, Hänninen OO. Fatty acid composition of erythrocyte, platelet, and serum lipids in strict vegans. Lipids. 1995 Apr;30(4):365-9. (Abstract) Raw food vegans. Not cited.
Craddock JC, Neale EP, Probst YC, Peoples GE. Algal supplementation of vegetarian eating patterns improves plasma and serum docosahexaenoic acid concentrations and omega-3 indices: a systematic literature review. J Hum Nutr Diet. 2017 Dec;30(6):693-699. The six studies included in this review are all summarized in DHA Supplementation in Vegans. Not cited.
Crawford MA. Docosahexaenoic acid in neural signaling systems. Nutr Health. 2006;18(3):263-76.
Fisher M, Levine PH, Weiner B, Ockene IS, Johnson B, Johnson MH, Natale AM, Vaudreuil CH, Hoogasian J. The effect of vegetarian diets on plasma lipid and platelet levels. Arch Intern Med. 1986 Jun;146(6):1193-7. No omega-3 data. Found higher LA but similar AA levels among vegans, lacto-ovo-vegetarians, and meat-eaters. Not cited.
Innis SM. Essential fatty acid transfer and fetal development. Placenta. 2005 Apr;26 Suppl A:S70-5.
Kris-Etherton PM, Hill AM. N-3 fatty acids: food or supplements? J Am Diet Assoc. 2008 Jul;108(7):1125-30. No abstract available. Not cited.
Lands WE, Morris A, Libelt B. Quantitative effects of dietary polyunsaturated fats on the composition of fatty acids in rat tissues. Lipids. 1990 Sep;25(9):505-16. Not cited above, but is citation #43 from Sarkadi-Nagy et al. (2004); mathematically complex paper which I couldn’t assess.
Li D, Sinclair A, Mann N, Turner A, Ball M, Kelly F, Abedin L, Wilson A. The association of diet and thrombotic risk factors in healthy male vegetarians and meat-eaters. Eur J Clin Nutr. 1999 Aug;53(8):612-9. Same measurements as provided in Li, 2002.
Li D, Turner A, Sinclair AJ. Relationship between platelet phospholipid FA and mean platelet volume in healthy men. Lipids. 2002 Sep;37(9):901-6. Same measurements as provided in Li, 1999.
Norris, J. Personal calculations. 2024. 1 teaspoon of dried chia seeds = 4 g (weighed on a food scale). USDA Nutrient database lists 28.35 g of dried chia seeds as having 5.05 g (5,050 mg) of ALA. 4 g * 5,050 mg ALA / 28.35 g = 712.52 mg ALA.
Peskin BS. Why fish oil fails: a comprehensive 21st century lipids-based physiologic analysis. J Lipids. 2014;2014:495761. (Retracted) Not cited.
Roshanai F, Sanders TA. Assessment of fatty acid intakes in vegans and omnivores. Hum Nutr Appl Nutr. 1984 Oct;38(5):345-54. Same study population as Sanders, 1992.
Sanders TA, Roshanai F. Platelet phospholipid fatty acid composition and function in vegans compared with age- and sex-matched omnivore controls. Eur J Clin Nutr. 1992 Nov;46(11):823-31. Same study population as Roshani, 1984.
Zhang Y, Jiao J. Reply to M Koch and MK Jensen. Am J Clin Nutr. 2016 Aug;104(2):537-8.




