

- UA
- EN
Кальцій
Джек Норріс, сертифікований дієтолог
Зміст
Основна інформація
Дорослі вегани повинні вживати 3 порції надійних джерел кальцію на день, тоді як підлітки — 4 порції. На зображенні нижче показано надійні джерела кальцію, доступні в Сполучених Штатах. На зображенні вказано кількість кожної страви, яка кваліфікується як одна порція.

На щастя, більшість рослинного молока збагачено кальцієм. І одним із моїх улюблених продуктів для отримання кальцію є кальцієвий тофу з високим вмістом кальцію та білка, які корисні для кісток. Якщо вам незручно щодня їсти продукти з високим вмістом кальцію, можна вживати добавку кальцію від 300 до 500 мг на день (дорослі повинні прагнути до нижньої межі діапазону, а підлітки — до вищої).
Силові вправи двічі на тиждень із підйомом помірної ваги є, мабуть, найнадійнішим способом зміцнення кісток. Ми закликаємо всіх включити такі заняття до свого розкладу. Поговоріть зі своїм лікарем про те, яка програма тренувань вам підходить.
Джерела кальцію рослинного походження
В електронній таблиці Вміст кальцію та оксалатів у рослинній їжі вказано вміст кальцію та відсоток його засвоєння з різних рослинних продуктів.
1 ч = 16 ст.л. = 236.6 мл [USDA]
Більшість даних про вміст кальцію в цій електронній таблиці отримано з бази даних поживних речовин Міністерства сільського господарства США (USDA), де вказано середнє значення проаналізованих зразків. Вміст кальцію в рослинній їжі певною мірою залежить від кількості кальцію в ґрунті [Weaver, 2013].
Рекомендована норма для кальцію базується на середньому поглинанні кальцію з їжі 25% (див. стор. 38 у [Dietary Reference Intakes, 2011]). Зі збільшенням дози кальцію відсоток його засвоєння зменшується. Окрім кількості самого кальцію, рівень оксалату в рослинних продуктах визначає те, скільки кальцію може бути засвоєно.
Офіційні рекомендації
Нижче наведено рекомендації щодо споживання кальцію для Великобританії та Сполучених Штатів. Ми рекомендуємо принаймні намагатися слідувати рекомендаціям Великобританії. Цілком безпечно приймати добавки кальцію, щоб компенсувати різницю між вашим звичайним раціоном і рекомендаціями.
Добова норма для кальцію на етикетках харчових продуктів становить 1300 мг.
Безпечність добавок кальцію
Деякі дослідження пов’язують вживання добавок кальцію з підвищеним ризиком серцево-судинних захворювань. Ці дослідження здебільшого виявили такий зв’язок серед людей, які значно перевищили рекомендовану норму для кальцію (більше інформації), а також сильніші наслідки у курців.
Проспективне когортне дослідження 2013 року в Швеції виявило, що вживання до 1300 мг кальцію на день не підвищує ризики серцево-судинних захворювань, але значно підвищений ризик дає вживання ≥1400 мг на день [Michaëlsson, 2013]. Інше дослідження, присвячене кальцифікації артерій, виявило крос-секційну кореляцію на початковому рівні, але не виявило проспективного зв’язку [Wang, 2010].
Фремінґемське дослідження (The Framingham Study) вимірювало споживання кальцію та спостерігало за учасниками протягом чотирьох років, після чого вимірювали ступінь кальцифікації їхніх артерій [Samelson, 2012]. Дослідники не виявили кореляції між споживанням кальцію та кальцифікацією артерій за умов вживання приблизно до 3000 мг на день у чоловіків чи жінок або добавок кальцію 500 мг на день або більше, порівняно з відсутністю добавок або вживанням кальцію до 500 мг на день. Див. також статтю Не потрібно турбуватися про кальцій і ваше серце з Tufts Health & Nutrition Letter (листопад 2019 р.).
Мультиетнічне дослідження атеросклерозу засвідчує зв’язок між кальцифікацією коронарних артерій (coronary artery calcification, CAC) і споживанням кальцію [Anderson, 2016, United States]. Дослідники спостерігали за учасниками, у яких не було CAC на початку дослідження, протягом 10 років. При коригуванні споживання кальцію використання добавки кальцію було пов’язане з підвищеним ризиком CAC (RR: 1,22, 95% CI: 1,07-1,39). Без коригування споживання кальцію використання харчових добавок було пов’язане з ледь значним підвищенням ризику CAC (RR: 1,12, 95% CI: 1,00-1,26, P=0,047). Ці дані свідчать про те, що використання деяких добавок кальцію може бути шкідливим, але, виходячи з результатів інших досліджень, ймовірно, при більш високому загальному споживанні кальцію.
Краще не споживати більше 1400 мг кальцію на день. Людям із хронічним захворюванням нирок варто поговорити зі своїми лікарями про переваги та недоліки добавок кальцію.
Колоректальний рак — ще одна проблема у контексті добавок кальцію. Як описано в статті про добавки кальцію та колоректальний рак, одне дослідження показало, що тривале використання 1200 мг добавки кальцію на день було пов’язане з підвищеним ризиком одного типу поліпа, який може призвести до колоректального раку. Цей підвищений ризик при вищому споживанні кальцію не спостерігався в інших дослідженнях, хоча інші дослідження не розглядали загальне споживання кальцію, а тільки окремі добавки. Автори цього дослідження рекомендують уникати добавок кальцію людям із зубчастими поліпами товстої або прямої кишки, особливо жінкам та курцям, [Crockett 2018].
Існує занепокоєння, що прийом добавок кальцію може підвищити ризик утворення каменів у нирках, але дослідження показали, що прийом добавок кальцію під час їжі може фактично знизити ризик утворення кальцієво-оксалатних каменів у нирках, найпоширенішої форми каменів. Для отримання додаткової інформації див. статтю про оксалат.
Деякі дослідження виявили підвищений ризик утворення каменів у нирках при прийомі високих доз кальцію та вітаміну D [Letavernier, 2018] [Avenell, 2014]. Прийом кальцію, який аналізувався у цих дослідженнях, становив 1000 мг на добу або більше [Lappe, 2017] [Jackson, 2006].
Отримувати достатню кількість кальцію важливо, проте не вживайте більше 1400 мг кальцію на день без лікарської рекомендації.
Дослідження кальцію та веганської дієти
Немає підстав вважати, що вегани захищені від остеопорозу краще, ніж люди з іншим харчуванням, тож їм варто намагатися відповідати рекомендаціям щодо споживання кальцію.
Рекомендована у США дієтична норма кальцію для дорослих становить від 1000 до 1200 мг на день залежно від статі та віку. Всесвітня організація охорони здоров’я пропонує подібні рекомендації [WHO, 2004]. Можна задовольнити рекомендації щодо споживання кальцію, споживаючи лише зелень (темну листову зелень - прим. ред.), проте середньостатистичний веган, ймовірно, не задовольнить рекомендації, якщо щодня не випиватиме склянку напою, збагаченого кальцієм, не з’їдатиме тофу з кальцієм або не прийматиме добавки.
Оскільки вегани не вживають молочні продукти, споживання кальцію в них зазвичай низьке. Посібник дієтолога щодо вегетаріанської дієти (2004) у Додатку G перелічує 45 досліджень, які аналізували споживання кальцію вегетаріанцями. Щоденне споживання кальцію в цих дослідженнях було таким:
Вегани: 500-600 мг
Лактоововегетаріанці: 800-900 мг
Невегетаріанці: 1000 мг
Лише одне дослідження включало добавки. У ньому добове споживання кальцію становило: 840 мг (чоловіки-вегани), 720 мг (чоловіки-невегетаріанці), 710 мг (жінки-веганки) і 855 мг (жінки-невегетаріанки).
Тваринний білок і остеопороз
Як ви бачите вище, споживання кальцію веганами, як правило, трохи нижче, ніж лактоововегетаріанцями чи невегетаріанцями, а також нижче за рекомендовану добову норму. Традиційно веганська спільнота реагує на це твердженнями про те, що остеопороз — це хвороба втрати кальцію з кісток, а не брак кальцію в раціоні. Це твердження ґрунтується на двох доказах.
Перший доказ: екологічні дослідження показали, що країни з найбільшим споживанням молочних продуктів (північна Європа та США) мають вищий відсоток випадків переломів стегна, ніж країни Азії та Африки, де споживають набагато менше молока.
Це можна пояснити другим доказом: дослідження показують, що після споживання тваринного білка люди виділяють із сечею велику кількість кальцію. Відповідно, вважається, що споживання кальцію не є важливим для запобігання остеопорозу і веганам не варто перейматися через відсутність тваринного білка в раціоні.
Давайте перевіримо ці докази.
Обсерваційні дослідження
Хоча це правда, що в азіатських країнах рівень переломів стегна нижчий, ніж у країнах з більшим споживанням молочних продуктів, виявилося, що показники переломів стегна можуть вводити в оману. Перше проспективне когортне дослідження, яке вимірює клінічно діагностовані переломи хребців в азіатському населенні, — Гонкозьке дослідження остеопорозу (Hong Kong Osteoporosis Study) — виявило, що при нижчій частоті переломів стегна в Гонконґу, порівняно зі Швецією, частота переломів хребців була вищою [Bow, 2012], як показано на зображенні нижче.
")
[Bow, 2012] стверджують:
“Спостережувані етнічні відмінності в частоті переломів можуть бути пов’язані з тим, що ризик перелому стегна залежить від ризику падіння, тоді як ризик перелому хребта здебільшого залежить від міцності кісток. Незважаючи на низький рівень переломів стегна серед нашої популяції, поширеність остеопорозу в жінок Гонконґу була вищою, ніж у білих жінок США (35,8% проти 20% відповідно), і так само серед чоловіків Гонконґу поширеність остеопорозу десь на 6% вища, ніж серед білих чоловіків США.”
Інакше кажучи, принаймні в цій групі людей із Гонконґу в китайців не виявлено нижчих показників остеопорозу.
[Darling et al. (2009)] провели систематичний огляд і метааналіз 28 досліджень білка і здоров’я кісток, включаючи перехресні, проспективні когортні та інтервенційні дослідження. Загалом було виявлено дуже мало доказів негативного впливу білка на мінеральну щільність кісткової тканини, при цьому більшість когортних досліджень повідомляли про відсутність будь-якого впливу або про позитивний вплив.
Одне дослідження показало значне збільшення ризику при збільшенні споживання тваринного білка та збільшення співвідношення тваринного білка по відношенню до рослинного. Три дослідження показали зниження відносного ризику перелому стегна зі збільшенням споживання тваринного, рослинного білка та загального його споживання. Два дослідження не виявили суттєвого зв’язку між споживанням тваринного білка та ризиком переломів, тоді як два інші дослідження не виявили зв’язку між загальним споживанням білка та ризиком переломів. Автори заявляли, що конфлікту інтересів не було.
[Shams-White, et al. (2017)] провели метааналіз 20 проспективних обсерваційних досліджень і 16 рандомізованих контрольованих досліджень і не виявили істотного зв’язку між харчовим білком і ризиком переломів. Існують деякі докази того, що більша кількість білка зменшує втрату кісткової маси в поперековому відділі хребта серед літніх людей. Дослідження було профінансовано компанією Egg Nutrition Center і Dairy Management Inc., яка, як стверджується, не брала жодної ролі в розробці, аналізі, інтерпретації чи представленні даних або результатів.
У французькому дослідженні (включеному в метааналіз Шемса-Вайта та ін.) [Dargent-Molina, 2008] виявили, що серед жінок із споживанням кальцію менше 400 мг на день споживання білка, який, як дослідники припустили, був переважно білком тваринного походження, підвищувало ризик переломів.
У шведському дослідженні [Michaëlsson 2014 et al. (2014)] виявили, що споживання молока корелювало з ранньою смертю як у чоловіків, так і у жінок, а також із переломами, особливо переломами стегна, у жінок. Незважаючи на статистичну значущість, відмінності не були достатньо значними, щоб вказувати на те, що молочні продукти відіграють помітну роль у ранній смертності або ризику переломів.
Метаболічні дослідження
Як згадувалося вище, існує теорія, що білок підвищує ризик остеопорозу, через те що збільшується втрата кальцію з сечею. Ця теорія полягає в тому, що білок, особливо через амінокислоти, що містять сірку, підвищує рівень кислоти в крові, яка, своєю чергою, потрапляє в сечу, збільшуючи кислотне навантаження на нирки. Щоб нейтралізувати цю кислоту, кальцій використовується як буфер, а потім виводиться разом із кислотою.
Було проведено величезну кількість досліджень білка та здоров’я кісток, і теорія про те, що білок викликає остеопороз, була спростована. Ось деякі з основних положень огляду клінічних випробувань на тему [Calvez, 2012]:
Багато клінічних випробувань показують, що додавання очищених білків до раціону збільшує виведення кальцію із сечею. Але коли люди вживають цільні продукти, цей ефект не є сильним. А фосфор, на який багаті м’ясо і молочні продукти, протидіє підвищенню вмісту кальцію в сечі на 40-65%.
Дієта з високим вмістом білка збільшує виділення кислоти із сечею, але з цим кислотно-буферна система організму може впоратися без потреби в кальції.
У дієті з низьким вмістом кальцію, а не з високим вмістом кальцію, більш високе споживання білка, ймовірно, збільшує рівень засвоєння кальцію з травного тракту, збільшуючи виділення кальцію з сечею.
Фрукти та овочі корисні для здоров’я кісток, ймовірно, завдяки високому вмісту калію та магнію. Це може призвести до плутанини в дослідженнях білка, оскільки дієти з високим вмістом білка часто містять мало фруктів і овочів.
Є докази того, що благотворний вплив білка на кістки спостерігається лише за умови адекватного споживання кальцію та вітаміну D.
Підтримка нормальної міцності та щільності кісток у процесі старіння залежить від здорової м’язової маси, яка залежить від достатнього споживання білка.
Збільшення рівня інсуліноподібного фактора росту 1 (IGF-1), найімовірніше, є механізмом покращення здоров’я кісток при більшому споживанні білка.
У цьому огляді роблять такий висновок:
Незважаючи на те, що дієти з високим вмістом білка викликають збільшення кислотності та виведення кальцію з сечею, вони, здається, не пов’язані з порушенням балансу кальцію, і жодні клінічні дані не підтверджують гіпотезу про шкідливий вплив дієти з високим вмістом білка на здоров’я кісток, за винятком випадків недостатнього споживання кальцію.
Інший метааналіз 2009 року виявив, що серед п’яти добре спланованих досліджень, які вимірювали баланс кальцію, екскреція кислоти не була пов’язана ні зі зниженням балансу кальцію, ні з маркером погіршення стану кісток [Fenton, 2009].
Причини остеопорозу
Якщо не тваринний білок викликає остеопороз, то що?
Генетика, ймовірно, відіграє значну роль у розвитку остеопорозу та, можливо, пов’язаного з цим рівня естрогену у жінок. Існують докази щодо певних факторів, які можна контролювати за допомогою способу життя та харчування.
Допомагають запобігти остеопорозу:
Силові вправи протягом усього життя
Більша маса тіла
Достатнє споживання кальцію, вітаміну D, вітаміну K, фосфору, калію, магнію та бору
Підвищує ризик остеопорозу:
Високе споживання натрію та кофеїну
Куріння
Занадто мале споживання білка
Надлишок вітаміну А (ретинолу, а не бета-каротину)
Можливо, дефіцит вітаміну B12
Кальцій і вітамін D
Коротка довідкова інформація: коли рівень кальцію в крові падає, виділяється паратиреоїдний гормон (ПТГ). ПТГ викликає вивільнення кальцію з кісток, таким чином підвищуючи низький рівень кальцію в крові. Остеопороз може бути наслідком хронічно високого рівня ПТГ.
Перетворення 25-гідроксивітаміну D на кальцитріол також певною мірою регулюється рівнями ПТГ [Groff, 2000]. Кальцитріол покращує рівень засвоєння кальцію та фосфору (іншого основного компонента кісток) із кишечника та зменшує рівень їхнього виведення із сечею. При цьому рівень кальцію в крові підвищується, а рівень ПТГ знижується.
Дослідження показали, що в середньому американці отримують достатньо кальцію. [Bischoff-Ferrari, et al. (2007)] провели метааналіз проспективних досліджень і рандомізованих контрольованих досліджень і виявили, що споживання кальцію та добавки кальцію не були пов’язані з меншим ризиком переломів стегна.
[Bolland, et al. (2015)] провели метааналіз 44 когортних досліджень і виявили, що кальцій, отриманий із їжі від 800 до 1000 мг на день, не пов’язаний з ризиком переломів, і немає жодних доказів того, що збільшення кальцію в цьому діапазоні або вище запобігає переломам. Винятком є те, що добавки кальцію та вітаміну D, як було встановлено, допомагають жінкам віком від 69 до 106 років, які зазвичай мають низьке споживання кальцію та низький рівень вітаміну D.
Вітамін В12 і мінеральна щільність кісток
Прийом вітаміну B12 також може бути важливим для мінеральної щільності кісток. Низький рівень вітаміну B12 може призвести до підвищення рівня гомоцистеїну, що може пошкодити кістки. Перехресне дослідження зі Словаччини порівнювало лактоововегетаріанок із всеїдними [Krivosikova, 2009].
Вегетаріанки мали нижчі рівні B12 (246 проти 302 пмоль/л) і вищі рівні гомоцистеїну (16,5 проти 12,5 мкмоль/л). Із чотирьох досліджених місць кісток у двох місцях у вегетаріанок була нижча мінеральна щільність кісток, ніж у всеїдних, а їхній вищий рівень гомоцистеїну мав негативну кореляцію з мінеральною щільністю кісток у трьох місцях. Кореляція мінеральної щільності кісткової тканини не була скоригована з урахуванням індексу маси тіла, який, хоч і не відрізнявся статистично між вегетаріанками та всеїдними (23,9 проти 25,0 відповідно), є важливим фактором, що впливає на мінеральну щільність кісткової тканини.
Перехресне дослідження, проведене в Німеччині, показало, що чоловіки-вегани та лактоововегетаріанці мали однакові показники обміну кісткової тканини, але вищі, ніж всеїдні [Herrmann, 2009]. У веганів був досить високий середній рівень метилмалонової кислоти — 727 нмоль/л, що свідчить про значний дефіцит вітаміну В12. Жоден із учасників не приймав добавки B12, кальцію або вітаміну D.
Після розподілу досліджуваних на дві групи на основі їхнього рівня B12 група з низьким вмістом B12 мала вищі маркери обміну кісткової тканини. Однак, оскільки майже всі люди в групі з низьким вмістом B12 були веганами або вегетаріанцями (62 з 63) і лише небагато веганів або вегетаріанців були в групі з достатнім рівнем B12 (6 із 66), не можна чітко стверджувати, що маркери посиленого обміну кісткової тканини зумовлені поганим рівнем B12 чи іншим фактором, загальним для веганів і вегетаріанців.
Селен і мінеральна щільність кісток
У проспективному дослідженні, проведеному у Великобританії за участі 1144 жінок у постменопаузі з нормальною функцією щитовидної залози, вищий рівень селену був пов’язаний із більшою мінеральною щільністю кісткової тканини [Hoag, 2012].
Хоча метаболізм селену бере участь у функціонуванні щитовидної залози, дослідження показало, що зв’язок між селеном і мінеральною щільністю кісткової тканини не залежить від функції щитовидної залози. Після 6 років спостереження не виявили зв’язку між рівнем селену та переломами кісток. Оскільки споживання селену може бути низьким у веганській дієті в деяких країнах, важливо, щоб вегани забезпечували собі надійне джерело селену (див. Селен).
Дослідження веганів
Мінеральна щільність кісток
Кілька невеликих перехресних досліджень показали, що вегани мають таку саму або трохи нижчу мінеральну щільність кісток, як і невегани [Barr, 1998] [Lau, 1998] [Parsons, 1997] [Ho-Pham, 2009a].
[Ho-Pham, et al. (2009b)] провели метааналіз мінеральної щільності кісткової тканини вегетаріанців та дійшли висновку, що «вегетаріанська дієта, особливо веганська, має помірний вплив на мінеральну щільність кісткової тканини, але навряд чи цей вплив призведе до клінічно суттєвого підвищення ризику переломів».
Данське дослідження показало, що у веганів (розмір вибірки=78) рівень паратгормону (ПТГ) і кісткової лужної фосфатази вищий, ніж у всеїдних (розмір вибірки=78) [Hansen, 2018]. ПТГ у веганів був у межах норми, тоді як кісткова лужна фотосфатаза могла бути дещо підвищена у невеликої кількості веганів. Незрозуміло, чи мали ці маркери клінічну значущість.
Кількісне ультразвукове дослідження
Кількісне ультразвукове дослідження — це метод непрямого вимірювання мінеральної щільності кісткової тканини.
[Menzel et al. (Germany, 2021)] провели цікаве перехресне дослідження відмінностей у стані кісток і харчування між 36 веганами та 36 всеїдними; кожна група складалася на 50% з жінок.
Дослідники вимірювали стан кісток за допомогою кількісного ультразвукового дослідження п’яткової кістки. Вони проаналізували дані за допомогою регресії зниженого рангу (reduced rank regression, RRR), у якій змішали веганів і всеїдних разом, щоб побачити, чи деякі кореляції, які вони виявили між поживними речовинами та здоров’ям кісток у веганів, також були виявлені у всеїдних (натякаючи, що ця кореляція серед веганів може виявляти причиново-наслідковий зв’язок).
Факторами харчування, найбільш пов’язаними зі здоров’ям кісток, були такі (у порядку важливості): лізин у плазмі крові, йод у сечі, тиреотропний гормон (ТТГ), селенопротеїн Р у плазмі, вітамін А у плазмі, лейцин у плазмі, жирні кислоти n-3 у плазмі, кальцій у сечі і магній, вітамін B6 у плазмі. Багато з цих факторів ми розглядаємо більш детально в статті Переломи кісток серед веганів Великобританії: наслідки та рекомендації.
UK Biobank (2023)
У великій проспективній британській когорті з майже 500 000 чоловіків і жінок вегетаріанці мали вищий ризик перелому стегна порівняно з тими, хто регулярно їсть м’ясо (HR: 1,50, 95% CI: 1,18-1,91), що еквівалентно скоригованій абсолютній різниці ризиків у 3,2 раза більшої кількості (95% CI: 1,2-5,8) переломів стегна на 1000 осіб протягом 10 років [Webster, 2023]. Дослідники описали цю різницю в абсолютному ризику як «помірну».
В аналізі, який відокремив веганів від лактоововегетаріанців, було лише 10 випадків переломів стегна серед веганів, але цього було достатньо, щоб досягти статистично значущої різниці порівняно з м’ясоїдами (HR: 3,26, 95% CI: 1,75- 6.08).
Різниця між індексом маси тіла вегетаріанців (25,6) і всеїдних (27,3) могла пояснити лише 28% різниці в ризиках перелому стегна. Споживання поживних речовин не оцінювалося.
Адвентистське дослідження здоров’я-2 (2021 та 2014)
[Thorpe et al. (2021)] опублікували звіт з Adventist Health Study-2, у якому порівнювали частоту переломів стегна в різних групах харчування лише серед білих учасників 45 років і старше (через їхнє загалом погане здоров’я кісток).
У жінок-веганок був вищий ризик перелому стегна порівняно з невегетаріанками (Коефіцієнт ризику: 1,55, Довірчий інтервал: 1,06-2,26). Ці результати були скориговані з урахуванням ваги та зросту, але не з урахуванням індексу маси тіла (ІМТ), тому важко зрозуміти, чи різниця пов’язана в основному з нижчим ІМТ веганок, який було виявлено в Adventist Health Study-2 (див. Маркери серцево-судинних захворювань у веганів: Звіт Адвентистського дослідження здоров’я 2 за 2013 рік).
Результати також були скориговані на загальне споживання кальцію та загальне споживання вітаміну D, але не на споживання білка. У таблиці нижче показано споживання речовин веганами та невегетаріанцями.
Після коригування на прийом добавок кальцію та вітаміну D дослідники виявили, що у веганів більше не виявлено більшого ризику перелому стегна. Висновок полягав у тому, що без добавок як вітаміну D, так і кальцію жінки-веганки мають високий ризик перелому стегна.
У попередньому звіті Adventist Health Study-2 (AHS-2) аналізувалися білі адвентисти сьомого дня, які проживають у США, та порівнювалося споживання багатьох різних продуктів і ризик перелому стегна після 5 років спостереження [Lousuebsakul-Matthews, 2014].
Дослідження показало, що вживання м’ясних альтернатив один раз на день або частіше (порівняно з рідше ніж раз на тиждень) було пов’язане зі зниженням ризику перелому стегна на 66% у вегетаріанців (0,34, 0,12-0,95). Вживання бобових один раз на день або частіше (порівняно з рідше ніж раз на тиждень) пов’язувалося зі зниженням ризику на 55% у вегетаріанців (0,45, 0,22-0,94).
EPIC-Oxford (2020 і 2007)
Звіт EPIC-Oxford [Tong, 2020] виявив вищий рівень переломів кісток серед веганів без будь-якого очевидного пояснення. Хоча вегани мали нижче середнє споживання кальцію (591 мг на день порівняно з ~1000 мг на день для інших харчових груп), було виявлено мало зв’язку між споживанням кальцію та вищим ризиком переломів. Див. Переломи кісток серед веганів Великобританії: наслідки та рекомендації.
Попередній аналіз EPIC-Oxford [Appleby, 2007] виявив, що у веганів частота переломів на 30% вища, ніж у м’ясоїдів (RR: 1,30, CI: 1,02-1,66) після поправки на куріння, алкоголь, індекс маси тіла, ходьбу, їзду на велосипеді, інтенсивні вправи, інші вправи, фізичну активність на роботі, сімейний стан, паритет(?) і замісну гормональну терапію.
Коли результати були скориговані на споживання кальцію, у веганів більше не виявлялася вища частота переломів. Серед досліджених, чий раціон містив ≥525 мг кальцію на день (це лише 55% веганів порівняно з приблизно 95% інших харчових груп), вегани мали такий же рівень переломів, як і люди з інших груп.
Автори дослідження UK Biobank вказують на обмеження цього звіту з Adventist Health Study-2: переломи стегна були визначені за допомогою опитувальників, заповнених власноруч, дані яких вибірково втрачалися для подальшого спостереження порівняно з лікарняними записами, які використовувалися в когортах Великобританії, описаних вище [Webster, 2023].
Буддійські черниці (В’єтнам, 2011)
[Ho-Pham et al. (2011)] досліджували 88 веганок і 93 всеїдних. Після двох років спостереження 5 веганок і 5 всеїдних отримали новий перелом хребта; не було виявлено істотної різниці між двома групами.
Анкети щодо харчування показали, що веганки споживали в середньому лише 1093 калорії, 36 г білка та 360 мг кальцію на день. Розрахована норма для жінок їхнього віку та статури становить близько 1600 калорій, що вказує на можливу недооцінку в анкетах. Черниці, які не були веганками, споживали 1429 калорій, 62 г білка та 590 мг кальцію на день, що здається більш правдоподібним.
Десять переломів у 181 жінки за два роки — це високий показник. Частота переломів хребців у жінок старше 65 років у Гонконґу та Японії становить 594 на 100 000 людинороків [Ho-Pham, 2009a]. Частота переломів у цьому дослідженні буддійських черниць становить 2762 на 100 000 людинороків. Переломи в дослідженні буддійських черниць визначалися рентгенівським обстеженням кожної досліджуваної, а не повідомленням про перелом, тож, імовірно, тут було виявлено більше переломів, ніж у дослідженні, яке отримало показник 594/100 000.
Таким чином, порівняно з буддистськими черницями, які не були вегетаріанками, черниці-веганки мали подібну частоту переломів хребців, але показники для обох груп видаються високими.
Бібліографія
___Calcium
by Jack Norris, RD
Contents
Essential Information
Vegan adults should eat 3 servings of good sources of calcium per day while teenagers should eat 4 servings. The image below shows good sources of calcium that are readily available in the United States. The image lists the amount of each food that qualifies as one serving.

Luckily, most plant-based milks are fortified with calcium. And one of my favorite foods for obtaining calcium is calcium-set tofu, which is high in calcium and protein, both of which are good for bones. If you find it inconvenient to eat foods high in calcium each day, a calcium supplement of 300 to 500 mg per day is another option, where adults should aim for the lower end of the range and teenagers should aim for the higher end.
Resistance exercise twice a week, involving lifting moderate weights, is possibly the most reliable way for people to increase the strength of their bones. We encourage everyone to follow such a program. Talk to your health professional about what program is right for you.
Plant Food Sources of Calcium
The spreadsheet Calcium and Oxalate Content of Plant Foods lists the amounts of calcium and absorption rates of various plant foods.

1 cup = 16 tsp. = 236.6 ml [USDA]
Most of the calcium amounts in that spreadsheet come from the USDA nutrient database, which lists an average of the samples they’ve analyzed. The amount of calcium in plant foods is somewhat dependent on the amount of calcium in the soil [Weaver, 2013].
The DRI for calcium is roughly based on an average absorption of calcium from foods of 25% (p. 38 in [Dietary Reference Intakes, 2011]). As a calcium dose increases, the percentage absorbed decreases. Beyond the size of the dose of calcium, the oxalate level in plant foods is the main determinant of how much calcium can be absorbed.
Official Recommendations
Below are the calcium intake recommendations for the United Kingdom and the United States. We recommend aiming to at least meet the U.K. recommendations. It’s safe to take a calcium supplement to make up the difference between your usual dietary intake and the recommendations.
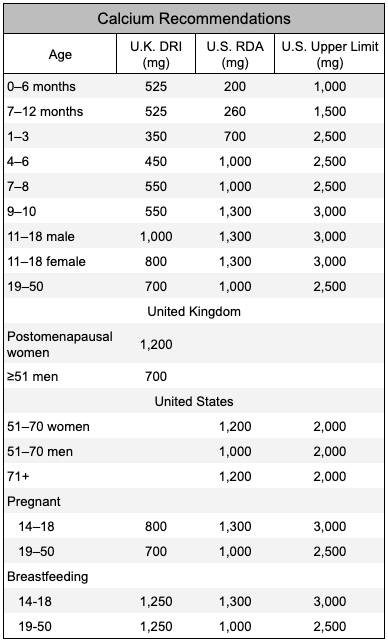
The Daily Value for calcium on food labels is 1,300 mg.
Safety of Calcium Supplements
Some research has linked calcium supplements with an increased risk of cardiovascular disease. These studies have mostly found a link in people getting well over the DRI for calcium (more info) with the effect stronger in smokers.
A 2013 prospective cohort study from Sweden found that there was no increased risk of up to 1,300 mg of calcium per day, but a significantly increased risk ≥1,400 mg per day [Michaelsson, 2013].
Another study looking at calcification of the arteries found a cross-sectional correlation at baseline, but no prospective association [Wang, 2010].
The Framingham Study measured calcium intakes and followed participants for four years at which time they measured the amount of calcification of their arteries [Samelson, 2012]. They found no correlation or trends with calcium intake and calcification of the arteries in amounts up to about 3,000 mg per day in either men or women or for calcium supplements of 500 mg per day or more compared to no supplements or up to 500 mg per day. See also No Need to Worry About Calcium and Your Heart from the Tufts Health & Nutrition Letter (November, 2019).
The Multi-Ethnic Study of Atherosclerosis reported on the association between coronary artery calcification (CAC) and calcium intake [Anderson, 2016, United States]. They followed participants free of CAC at baseline for 10 years. When adjusting for calcium intake, calcium supplement use was associated with an increased risk of CAC (RR: 1.22, 95% CI: 1.07-1.39). When not adjusting for calcium intake, supplement use was associated with a barely significant increased risk of CAC (RR: 1.12, 95% CI: 1.00-1.26, P=0.047). These findings suggest that some calcium supplement use may be harmful, but, based on other research findings, likely at higher total calcium intakes.
To be safe, it might be best not to increase calcium intake above 1,400 mg per day. People with chronic kidney disease should talk to their physicians about the pros and cons of calcium supplements.
Colorectal cancer is another concern with regard to calcium supplements. As described in Calcium Supplements and Colorectal Cancer, one study found that long-term use of a 1,200 mg per day calcium supplement was associated with an increased risk of one type of polyp that can lead to colorectal cancer. This increased risk with higher calcium intakes was not seen in other studies although the other studies didn’t look at total calcium intake rather than supplements specifically. The authors of this study suggest that those with serrated polyps of the colon or rectum, especially women and smokers, avoid calcium supplements [Crockett 2018].
There’s been a concern that taking calcium supplements can increase the risk of kidney stones, but for the most part, research has shown that taking calcium supplements with meals can actually reduce the risk of calcium-oxalate kidney stones, the most common form of stone. For more information, see the article Oxalate.
Some studies have found an increased risk of kidney stones when taking both high-dose calcium and vitamin D supplements [Letavernier, 2018] [Avenell, 2014]. The amount of calcium taken in these studies tends to be 1,000 mg or higher [Lappe, 2017] [Jackson, 2006].
Although it’s important to get enough calcium, don’t ingest more than 1,400 mg of calcium per day without the supervision of a health professional.
Research on Calcium and Vegan Diets
There’s no reason to think that vegans are protected from osteoporosis more than other diet groups and they should strive to meet calcium recommendations.
The U.S. Recommended Dietary Allowance for calcium for adults is 1,000 to 1,200 mg per day depending on sex and age. The World Health Organization has similar recommendations [WHO, 2004]. Although it’s possible to meet calcium recommendations by eating greens alone, the average vegan probably won’t meet recommendations without drinking a glass of a calcium-fortified beverage each day, eating calcium-set tofu, or taking a supplement.
Because vegans don’t eat dairy products, their calcium intakes tend to be low. The Dietitian’s Guide to Vegetarian Diets (2004) lists 45 studies that have surveyed vegetarian calcium intakes in Appendix G. The daily calcium intakes in these studies are about:
Vegans: 500-600 mg
Lacto-ovo vegetarians: 800-900 mg
Non-vegetarians: 1,000 mg
Only one study included supplements. In it, daily calcium intakes were: 840 mg (vegan males), 720 mg (non-vegetarian males), 710 mg (vegan females), and 855 mg (non-vegetarian females).
Animal Protein and Osteoporosis
As you can see above, the calcium intake of vegans tends to be quite a bit lower than lacto-ovo vegetarians, non-vegetarians, and the RDA. Traditionally, the vegan community has responded to this by saying osteoporosis is a disease of calcium loss from the bones, not a lack of calcium in the diet. This was based on two pieces of evidence.
The first piece is that ecological studies have shown that the countries with the highest intakes of dairy products (northern Europe and the USA) have higher rates of hip fractures than do Asian and African countries where much less milk is consumed.
This can be explained by the second piece of evidence which is that studies show that after ingesting animal protein, people urinate large amounts of calcium. Therefore, the thinking goes, calcium intake isn’t important for preventing osteoporosis and vegans are protected due to the lack of animal protein in their diets.
Let’s examine this evidence.
Observational Studies
While it’s true that Asian countries have lower rates of hip fractures than do higher dairy-consuming countries, it turns out that hip fracture rates can be misleading. The first prospective cohort study measuring clinically diagnosed vertebral fractures in an Asian population, the Hong Kong Osteoporosis Study, found that while hip fracture rates were lower in Hong Kong than Sweden, vertebral fracture rates were higher [Bow, 2012], as shown in the image below.

[Bow, 2012] state:
“The observed ethnic differences in fracture incidences may be due to the fact that hip fracture risk was affected by fall risk, whereas the risk of vertebral fracture mostly depends on bone strength. Despite the low hip fracture rate in our population, Hong Kong women had a higher prevalence of osteoporosis than US Caucasian women (35.8% vs. 20%, respectively) and a similar prevalence of about 6% in Hong Kong and US Caucasian men.”
In other words, at least in this group of people from Hong Kong, the Chinese don’t have lower rates of osteoporosis.
[Darling et al. (2009)] conducted a systematic review and meta-analysis of 28 studies on protein and bone health including cross-sectional, prospective cohort, and intervention trials. Overall, there was very little evidence of a negative influence of protein intake on bone mineral density (BMD) with most cohort studies reporting either no influence or a positive influence.
One study reported a significant increase in risk with increasing animal protein intake and increasing animal to vegetable protein ratio. Three studies found a decreased relative risk of hip fracture with increasing animal, total, and vegetable protein intakes. Two studies found no significant association of animal protein with fracture risk, whereas 2 studies found no association of total protein intake with fracture risk. The authors declared no conflict of interest.
[Shams-White, et al. (2017)] conducted a meta-analysis of 20 prospective observational studies and 16 randomized controlled trials and found no significant association between dietary protein and fracture risk. There was some evidence that more protein reduced bone loss of the lumbar spine among older adults. The study was supported by the Egg Nutrition Center and Dairy Management Inc. who were said not to have had any role in the design, analysis, interpretation, or presentation of the data or the results.
In a study from France (included in the meta-analysis by Shams-White et al.), [Dargent-Molina, 2008] found that among women with calcium intakes lower than 400 mg/day, protein intake, which they suggested was mostly animal protein, increased the risk of fracture.
In a study from Sweden, [Michaelsson 2014 et al. (2014)] found that milk consumption was positively associated with early death in both men and women, as well as fractures, especially hip fractures, in women. While statistically significant, differences weren’t large enough to indicate dairy plays more than a small role in early death or fractures.
Metabolic Studies
As mentioned above, there is a theory that protein increases osteoporosis by increasing a loss of calcium through the urine. The idea is that protein, especially through the sulfur-containing amino acids, increases the acid in the blood which, in turn, gets shuttled to the urine, increasing the renal acid load. In order to neutralize that acid, calcium is used as a buffer and then urinated out with the acid.
There has been an enormous amount of research on protein and bone health and this view of protein causing osteoporosis has been refuted. Here are some of the main points of a 2012 literature review [Calvez, 2012] of clinical trials on the subject:
Many clinical trials show that adding purified proteins to the diet increases calcium excretion through the urine. But when whole foods are eaten, this effect is not strong. And phosphorus, in which meat and dairy are rich, counteracts the increase of calcium in the urine between 40 and 65%.
High protein diets increase acid excretion in the urine, but this can be handled by the body’s acid buffer system without the need for calcium.
In low-calcium, but not high-calcium diets, higher protein intakes probably increase calcium absorption from the digestive tract causing an increase in calcium excretion in the urine.
Fruits and vegetables are beneficial to bone health, probably due to their high potassium and magnesium content. This could cause confounding in protein studies because diets high in protein are often low in fruits and vegetables.
There is some evidence that a beneficial effect of protein on bones is only seen when calcium intake and vitamin D status is adequate.
Maintenance of adequate bone strength and density with aging is dependent on adequate muscle mass which is dependent on adequate intake of protein.
An increase in IGF-1 is most likely the mechanism for increased bone health with higher protein intakes.
They conclude:
Although HP [high protein] diets induce an increase in net acid and urinary calcium excretion, they do not seem to be linked to impaired calcium balance and no clinical data support the hypothesis of a detrimental effect of HP diet on bone health, except in the context of inadequate calcium supply.
Another 2009 meta-analysis found that among five well-designed studies measuring calcium balance, net acid excretion was not associated with either decreased calcium balance or a marker of bone deterioration [Fenton, 2009].
Causes of Osteoporosis?
If animal protein doesn’t cause osteoporosis, what does?
Genetics likely play a strong role in osteoporosis, and, possibly related, estrogen levels in women. Among factors that can be controlled by lifestyle and diet, there has been evidence for the following:
Helps prevent:
Weight-bearing exercise throughout one’s lifetime
Higher body weight
Adequate intake of calcium, vitamin D, vitamin K, phosphorus, potassium, magnesium, and boron
Contributes to:
High sodium and caffeine intake
Smoking
Too little protein
Excessive vitamin A (retinol, not beta-carotene)
Possibly vitamin B12 deficiency
Calcium and Vitamin D
Some background: When calcium levels in the blood drop, parathyroid hormone (PTH) is released. PTH causes calcium to be released from the bones, thus raising the low calcium levels in the blood. Osteoporosis may result from chronically high levels of PTH.
The conversion of 25-hydroxyvitamin D to calcitriol is also somewhat regulated by PTH levels [Groff, 2000]. Calcitriol increases absorption of calcium and phosphorus (another major component of bones) from the intestines and decreases their excretion in the urine. In so doing, calcium levels in the blood rise and PTH levels drop.
Research has shown that, on average, Americans are getting enough calcium. [Bischoff-Ferrari, et al. (2007)] conducted a meta-analysis of prospective studies and randomized controlled trials and found that calcium intake and calcium supplements were not associated with a lower risk for hip fractures.
[Bolland, et al. (2015)] conducted a meta-analysis of 44 cohort studies and found that dietary calcium between about 800 to 1,000 mg per day isn’t associated with risk of fracture, and there’s no evidence that increasing dietary calcium within that range or higher prevents fractures. An exception is that calcium and vitamin D supplements have been found to help women aged 69 to 106 years old who normally have low calcium intake and poor vitamin D status.
Vitamin B12 and Bone Mineral Density
Taking vitamin B12 might also be important for bone mineral density.
Low vitamin B12 status can result in elevated homocysteine which might harm bones. A cross-sectional study from Slovakia compared lacto-ovo-vegetarian women to omnivores [Krivosikova, 2009].
The vegetarians had lower B12 levels (246 vs. 302 pmol/l) and higher homocysteine levels (16.5 vs. 12.5 µmol/l). In the four bone locations examined, vegetarians had lower bone mineral density than omnivores in two locations, and their higher homocysteine levels were negatively associated with bone mineral density in three locations. The bone mineral density associations appeared not to be adjusted for body mass index which, while not statistically different between the vegetarians and omnivores (23.9 vs. 25.0, respectively), is an important factor impacting bone mineral density.
A cross-sectional study from Germany found that male vegans and lacto-ovo-vegetarians had similar markers of bone turnover to each other, but higher markers than male omnivores [Herrmann, 2009]. The vegans had a rather high average methylmalonic acid level of 727 nmol/l, indicative of significant vitamin B12 deficiency. None of the participants were taking B12, calcium, or vitamin D supplements.
Upon stratifying the subjects into two groups based on their B12 status, the group with poor B12 status had higher markers of bone turnover. However, since almost all the people in the poor B12 status group were vegan or vegetarian (62 out of 63), and few vegans or vegetarians were in the replete B12 group (6 out of 66), it’s not clear that the increased bone turnover markers were due to poor B12 status or some other factor common to vegans and vegetarians.
Selenium and Bone Mineral Density
In a prospective study from the U.K. of 1,144 post-menopausal women with normal thyroid function, higher selenium levels were associated with greater bone mineral density [Hoag, 2012].
Although selenium metabolism is involved in thyroid function, the study found that the associations between selenium and bone mineral density were independent of thyroid function. After 6 years of follow-up, selenium levels were not associated with bone fractures. Because selenium intakes can be low in vegan diets in some countries, it’s important that vegans in those countries ensure an adequate source (see Selenium).
Research on Vegans
Bone Mineral Density
A number of small, cross-sectional studies have shown vegans to have the same or slightly lower bone mineral density as non-vegans [Barr, 1998] [Lau, 1998] [Parsons, 1997] [Ho-Pham, 2009a].
[Ho-Pham, et al. (2009b)] conducted a meta-analysis looking at the bone mineral density of vegetarians, concluding that “[T]here is a modest effect of vegetarian diets, particularly a vegan diet, on [bone mineral density], but the effect size is unlikely to result in a clinically important increase in fracture risk.”
A Denmark study found that vegans (n=78) had higher levels of parathyroid hormone (PTH) and bone-specific alkaline phosphatase (BAP) than omnivores (n=78) [Hansen, 2018]. Vegan PTH was within the normal range while BAP might have been slightly elevated for a small number of vegans. It’s not clear if these markers were of clinical significance.
Quantitative Ultrasound
Quantitative ultrasound (QUS) is a method for indirectly measuring bone mineral density.
[Menzel et al. (Germany, 2021)] performed an interesting cross-sectional study of the differences in bone and nutrition status between 36 vegans and 36 omnivores; each group was 50% female.
They measured bone status using quantitative ultrasound of the calcaneus bone. They analyzed the data using reduced rank regression (RRR) in which they mixed vegans and omnivores together to see if some of the associations they found between nutrient status and bone health in vegans were also found in the omnivores (suggesting more strongly that they might be causal among vegans).
The nutrition factors most associated with bone health, in order of importance, were: plasma lysine, urinary iodine, thyroid-stimulating hormone (TSH), plasma selenoprotein P, plasma vitamin A, plasma leucine, plasma n-3 fatty acids, urinary calcium and magnesium, and plasma vitamin B6. We examine many of these factors in more detail in the article Bone Fractures among U.K. Vegans: Implications and Recommendations.
UK Biobank (2023)
In a large prospective British cohort of almost 500,000 men and women, vegetarians were at a higher risk of hip fracture compared to regular meat-eaters (HR 1.50, 95% CI: 1.18-1.91), the equivalent of an adjusted absolute risk difference of 3.2 (95% CI: 1.2-5.8) more hip fractures per 1,000 people over a 10 year period [Webster, 2023]. The researchers described this difference in absolute risk as “modest.”
In an analysis separating the vegans from lacto-ovo-vegetarians, there were only 10 cases of hip fractures among vegans but that was enough to reach a statistically significant difference as compared to regular meat-eaters (HR 3.26, 95% CI: 1.75-6.08).
Differences between the body mass index of the vegetarians (25.6) and meat-eaters (27.3) could only explain 28% of the difference in hip fracture risk. Nutrient intake wasn’t assessed.
Adventist Health Study-2 (2021 & 2014)
[Thorpe et al. (2021)] published a report from the Adventist Health Study-2 comparing hip fracture rates of different diet groups among white participants only (due to their generally poorer bone health) who were 45 years or older.
Female vegans had a higher risk of hip fracture compared to non-vegetarians (HR 1.55, CI 1.06-2.26). These findings were adjusted for weight and height, but not for body mass index (BMI), so it’s hard to know if the difference is mainly due to the lower BMI of vegans which has been found in the Adventist Health Study-2 (see Cardiovascular Disease Markers of Vegans: 2013 Report from Adventist Health Study-2).
The findings were also adjusted for total calcium intake and total vitamin D intake, but not for protein intake. The table below shows the intakes of vegans and nonvegetarians.
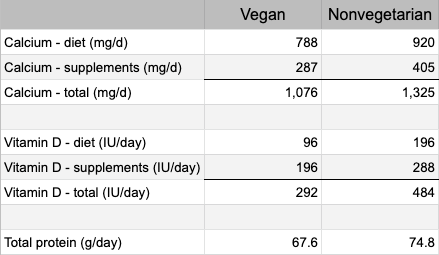
After adjusting for calcium and vitamin D supplementation together, the researchers found that the vegans no longer had a higher risk of hip fracture. Their conclusion was that without supplementation of both vitamin D and calcium, female vegans are at high risk of hip fracture.
A previous report from Adventist Health Study-2 (AHS-2) examined caucasian Seventh-day Adventists living in the USA, comparing the intakes of many different foods and hip fracture risk after 5 years of follow-up [Lousuebsakul-Matthews, 2014].
The study found that eating meat alternatives once a day or more (compared to less than once per week) was associated with a 66% reduced risk of hip fracture in the vegetarians (0.34, 0.12-0.95). Eating legumes once per day or more (compared to less than once per week) was associated with a 55% reduced risk in vegetarians (0.45, 0.22-0.94).
EPIC-Oxford (2020 & 2007)
A report from EPIC-Oxford [Tong, 2020] found a higher rate of bone fracture among vegans without any obvious explanation. Although vegans had a lower average calcium intake (591 mg/day compared to ~1,000 mg/day for other diet groups), there was little association between calcium intakes and a higher risk of fracture. See Bone Fractures among U.K. Vegans: Implications and Recommendations for more information.
A previous analysis from EPIC-Oxford [Appleby, 2007] found vegans to have a 30% higher fracture rate than meat-eaters (RR 1.30, CI 1.02-1.66) after adjusting for smoking, alcohol, body mass index, walking, cycling, vigorous exercise, other exercise, physical activity at work, marital status, parity and hormone replacement therapy.
When the results were adjusted for calcium intake, the vegans no longer had a higher fracture rate. Among the subjects whose diets contained ≥525 mg of calcium a day (only 55% of the vegans compared to about 95% of the other diet groups), vegans had the same fracture rates as the other diet groups.
The authors of the UK Biobank study point out a limitation of this report from Adventist Health Study-2 which is that hip fractures were identified from self-reported questionnaires prone to selective loss to follow-up as compared to hospital records used in the UK cohorts described above [Webster, 2023].
Buddhist Nuns (Vietnam, 2011)
[Ho-Pham et al. (2011)] studied 88 vegans and 93 omnivores. After two years of follow-up, 5 vegans and 5 omnivores had sustained a new vertebral fracture; there was no significant difference between the two groups.
Food questionnaires indicated that the vegans were only eating an average of 1,093 calories, 36 g of protein, and 360 mg of calcium per day. The estimated energy requirement for women their age and size is about 1,600 calories indicating possible underestimation. The non-vegan nuns had intakes of 1,429 calories, 62 g of protein, and 590 mg of calcium per day which seems more plausible.
Ten fractures in 181 women in two years is high. The rate of vertebral fracture in women over 65 in Hong Kong and Japan is 594/100,000 person-years [Ho-Pham, 2009a]. The fracture rate in this Buddhist nun study works out to be 2,762/100,000 person-years. The fractures in the Buddhist nun study were determined by x-raying each subject, rather than reporting a bone break, and would likely find more fractures than the study determining the 594/100,000 rate.
In summary, compared to non-vegetarian Buddhist nuns, vegan nuns had a similar rate of vertebral fractures, but it appears that the rates for both groups were high.
Bibliography
___Groff J, Gropper S. Advanced Nutrition and Human Metabolism, 3rd ed. Wadsworth: 2000.
Ho-Pham 2009a. Ho-Pham LT, Nguyen PL, Le TT, Doan TA, Tran NT, Le TA, Nguyen TV. Veganism, bone mineral density, and body composition: a study in Buddhist nuns. Osteoporos Int. 2009 Apr 7. (Epub ahead of print)
Ho-Pham 2009b. Ho-Pham LT, Nguyen ND, Nguyen TV. Effect of vegetarian diets on bone mineral density: a Bayesian meta-analysis. Am J Clin Nutr. 2009 Oct;90(4):943-50.
Wang TK, Bolland MJ, van Pelt NC, Horne AM, Mason BH, Ames RW, Grey AB, Ruygrok PN, Gamble GD, Reid IR. Relationships between vascular calcification, calcium metabolism, bone density, and fractures. J Bone Miner Res. 2010 Dec;25(12):2777-85. Erratum in: J Bone Miner Res. 2011 Feb;26(2):439. The erratum listed for this abstract appears to itself be an erratum as it doesn’t apply to this paper.
Weaver 2013. Correspondence from Connie M. Weaver, PhD, Purdue University, Nutrition Science. September 2013.




