

- UA
- EN
Коферментні добавки: Метилкобаламін та аденозилкобаламін
Зміст
Резюме
Ціанокобаламін - це добре вивчена, надійна, недорога форма вітаміну В12, хоча вона містить молекулу ціаніду, яка в нормальних кількостях для більшості людей є фізіологічно не суттєвою. Багато нетрадиційних лікарів і компаній, що виробляють харчові добавки, пропагують коферментні форми В12 - метилкобаламін і аденозилкобаламін. Норми щодо цих альтернативних форм повністю не з'ясовані, і загальне рекомендоване дозування для них - 1 000 мкг/добу.
Вступ
Існує чотири форми вітаміну B12, що відрізняються боковою групою, приєднаною до молекули кобаламіну:
Аденозилкобаламін
Ціанокобаламін
Гідроксокобаламін
Метилкобаламін
Метилкобаламін та аденозилкобаламін представляють собою дві форми вітаміну B12, що є коферментами: організм вимагає кожного з них для різних реакцій.
Ціанокобаламін зазвичай зустрічається в добавках і збагачених продуктах. Він найбільш стійкий, тому що бокова група, ціанід, має найсильнішу прив'язку до молекули кобаламіну.
Гідроксокобаламін зазвичай застосовується для ін'єкцій B12, а бокова гідроксильна група має найменше тяжіння до молекули кобаламіну.
Аденозилкобаламін є технічно 5'-дезокси-5-аденозилкобаламіном, а також відомий як дибенкозид, кобамамид і кобінамид.
Коферментна форма добавок B12, аденозилкобаламін та метилкобаламін, іноді рекламуються як переважаючі над ціанокобаламіном, із двох причин:
Ціанокобаламін містить молекулу ціаніду.
Тіло повинно перетворити ціанокобаламін в аденозилкобаламін та метилкобаламін, перш ніж використовувати його.
Інші вважають, що ціанокобаламін – найкращий вибір для більшості людей, оскільки це найбільш стабільна форма, яка вже добре вивчена. Доведено, що вона підвищує рівень вітаміну B12, а також є найпоширенішою та найдешевшою.
Давайте розглянемо твердження на користь коферментних форм.
Ціанід
Безпечність ціанокобаламіну викликала стурбованість тим, що ціанід є компонентом ціанокобаламіну, а ціанідна молекула видаляється із ціанокобаламіну при використанні її клітинами. Ціанід також міститься в багатьох фруктах і овочах, тому люди завжди ковтають невелику кількість ціаніду, і, як у більшості фруктів і овочів, кількість ціаніду в ціанокобаламіні вважається фізіологічно незначною.
Для отримання додаткової інформації див. наш детальний аналіз у розділі "Вітамін В12 та ціанід".
Ефективність
У статті 2015 року [Obeid та інші] передбачається, що люди не отримують більше користі від коферментних форм, тому що для всіх форм, за винятком використовуваного в ін'єкціях гідроксокобаламін, бокові групи повинні бути від'єднані цільової клітиною, перш ніж необхідна бокова група буде приєднана до відповідної коферментної форми. Люди з генетичними дефектами метаболізму вітаміну B12 можуть скористатися ін'єкціями гідроксокобаламіну.
Цитата:
"Наразі в нас немає достатньо доказів того, що переваги використання метилкобаламіну або аденозилкобаламіну переважають використання ціанокобаламіну або гідроксокобаламіну з позицій біодоступності, біохімічних ефектів або клінічної ефективності. Існує невизначеність щодо заявлених переваг коферментних форм [B12] для профілактики і лікування дефіциту [B12]. Однак гідроксокобаламін може бути найкращим попередником (прекурсором) кофакторів, особливо в спадкових порушеннях метаболічного перетворення кобаламіну. Ціанокобаламін є більш стабільною та недорогою формою, яка, мабуть, найкраще підходить для перорального прийому та парентерального [внутрішньовенного] лікування."
Люди з генетичними дефектами метаболізму вітаміну В12 можуть отримати користь від ін'єкцій гідроксокобаламіну; Obeid et al. більш детально описують ці генетичні дефекти у своїй статті.
Абсорбція
Деякі дослідники сумніваються в тому, чи є коферментні добавки стабільними в пероральній формі, і зазвичай рекомендують набагато вищі дозування метилкобаламіну – 1000 мкг/день.
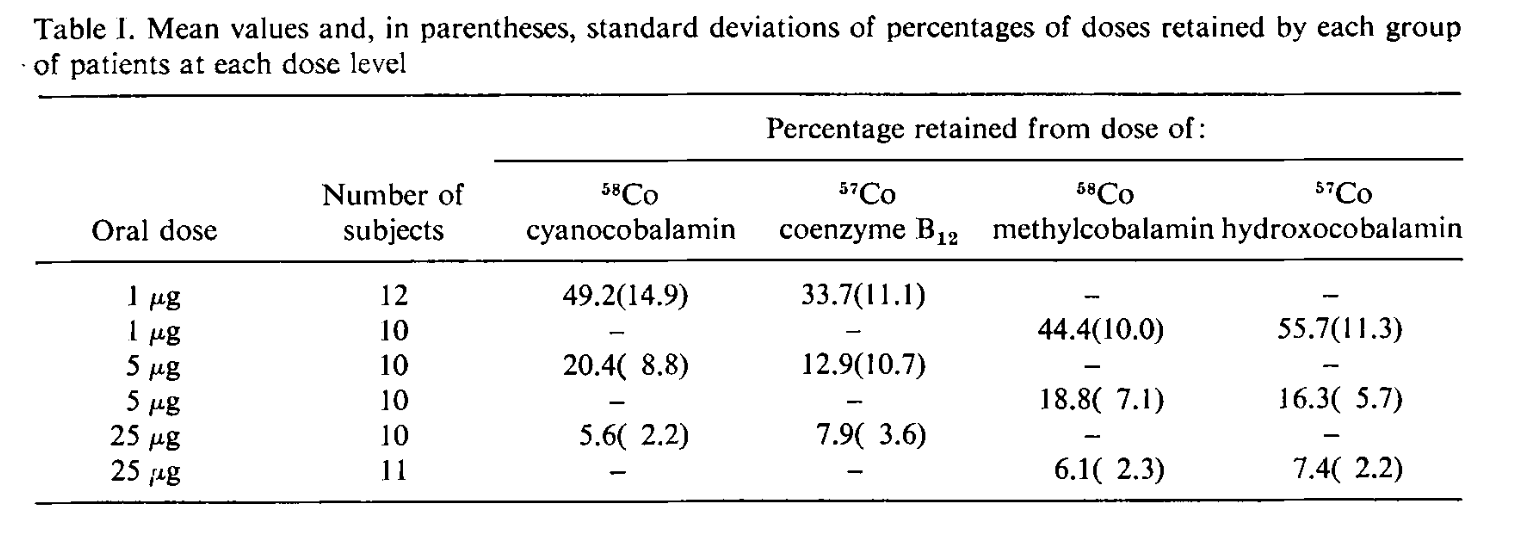
Дослідження 1971 року показало, що при дозуваннях в 1 мкг, 5 мкг і 25 мкг ціанокобаламін, гідроксокобаламін, метилкобаламін і аденозилкобаламін поглиналися приблизно з тією ж швидкістю [Adams, 1971].
Таблиця показників абсорбції:
Таблиця 1. Середнє значення, що утримується кожною групою пацієнтів, для кожного значення дозування (в дужках – стандартні відхилення в процентах)
Дослідження, проведене в 1973 році, передбачає, що після абсорбції метилкобаламін може зберігатися в організмі краще, ніж ціанокобаламін [Okuda, 1973].
Клінічне випробування в Кореї в 2011 році показало, що 1500 мкг/день метилкобаламіну підвищує рівень вітаміну B12, зменшує або усуває неврологічні симптоми дефіциту B12 і знижує рівень гомоцистеїну [Kim, 2011]. У дослідженні брали участь люди з гастректомією, а отже із мальабсорбцією вітаміну B12, з чого можна припустити, що для більшості людей 1500 мкг/день – більш ніж достатньо.
У цьому дослідженні не було контрольної групи, яка отримувала ціанокобаламін.
Я не знаю клінічних випробувань різних форм вітаміну B12 відносно одна одної серед населення в цілому, більшість людей, здається, чинить правильно, використовуючи ціанокобаламін.
Деякі люди з хронічною втомою відзначають, що отримують більше допомоги від аденозилкобаламіну, ніж від метилкобаламіну або ціанокобаламіну (більше інформації), тоді як інші люди повідомляють про поліпшення самопочуття тільки при прийнятті коферментних форм вітаміну B12 (метилкобаламіну і аденозилкобаламіну).
Це може бути реальним ефектом, але також може бути наслідком ефекту плацебо або прийняття більшої кількості B12 з ненавмисною протидією мальабсорбції.
Метилкобаламін та дослідження його впливу на веганів
Дональдсон [Donaldson (2000, USA)] вивчав трьох веганів з підвищеним рівнем метилмалоновой кислоти (ММК), які вживали (розсмоктували під язиком) 0,5-1 таблетки метилкобаламіну 2 рази на добу протягом 3 тижнів. Листування з автором (21 березня 2002) підтвердило, що одна таблетка містила 1000 мкг метилкобаламіну.
У двох з трьох випробовуваних рівень ММК нормалізувався, у третього учасника залишилося невелике перевищення 4,1 мкг/мг креатиніну (нормальне значення <4.0 мкг/мг креатиніну). Таким чином, при вживанні 1000-2000 мкг/день спостерігається високий рівень абсорбції метилкобаламіну, достатній, щоб поліпшити рівень вітаміну B12 у деяких веганів. Крім того, це означає, що метилкобаламін конвертувався в аденозилкобаламін для використання в процесах перетворень ММК.
Перехресне дослідження з Румунії
Перехресне дослідження, проведене в Румунії, показало, що вегани, які приймали ціанокобаламін, мали вищі рівні голотранскобаламіну, ніж ті, хто приймав метилкобаламін (150 пмоль/л і 78,5 пмоль/л відповідно; p-value=0,030; [Zugrav et al, 2021]). Однак ті, хто приймав метилкобаламін, отримували менше добавок, і їхня кількість була різною.
Рівень холотранскобаламіну 78,5 пмоль/л значно перевищує мінімальний здоровий діапазон, що свідчить про те, що режим прийому метилкобаламіну був адекватним. Середня доза для тих, хто приймав ціанокобаламін і метилкобаламін, становила 582 мкг і 988 мкг відповідно.
Частота прийому метилкобаламіну становила 21% щодня, 36% двічі на тиждень і 43% один раз на тиждень. Без оцінки рівнів ММА та більш точного співставлення значень з кількістю та частотою прийому неможливо визначити надійний режим прийому.
Тематичне дослідження з Німеччини
[Storz et al. (2024, Germany)] повідомили про клінічний випадок чоловіка середнього віку, який приймав одноразову пероральну дозу 500 мкг метилкобаламіну в середньому 3-4 рази на тиждень протягом багатьох років. Рівень вітаміну B12 у нього був здоровим і становив 303 пмоль/л (409 пг/мл), а рівень гомоцистеїну – 11,7 мкмоль/л (рівень вище 12 мкмоль/л вважається нездоровим).
Випадок з життя вегана
Я отримав таке повідомлення у 2011 році:
“Я приймав 500 мкг метилкобаламіну протягом багатьох років, не знаючи, що дозування вітаміну B12 (25-100 мкг щодня) призначаються тільки для ціанокобаламіну. Так, близько тижня тому я почав приймати 1000-2000 мкг метилкобаламіну замість 500 мкг і відчуваю різницю!”
Слід зазначити, що ця людина, можливо, страждала на мальабсорбцію будь-якої форми B12 і мала схожий досвід з ціанокобаламіном.
Гідроксокобаламін
Гідроксокобаламін – це одна з форм вітаміну B12, яка зазвичай зустрічається в продуктах харчування. Існує не так багато добавок цієї форми для перорального прийому, як правило, її використовують у вигляді ін'єкцій. Одне дослідження показує, що після ін'єкцій гідроксокобаламін зберігається в організмі краще, ніж ціанокобаламін [Tudhope, 1967].
Використана література
___Coenzyme Supplements: Methylcobalamin and Adenosylcobalamin
Contents
Summary
Cyanocobalamin is a well-studied, reliable, inexpensive form of vitamin B12, though it does contain a molecule of cyanide, which, in normal amounts, should be physiologically inconsequential for most people. Many alternative health practitioners and supplement companies promote the coenzyme forms of B12, methylcobalamin and adenosylcobalamin. Requirements for these alternative forms have not been fully elucidated and common recommendations are for 1,000 µg/day.
Introduction
There are four forms of vitamin B12, differentiated by the side group attached to the cobalamin molecule:
Adenosylcobalamin
Cyanocobalamin
Hydroxocobalamin
Methylcobalamin
Methylcobalamin and adenosylcobalamin are the two forms of vitamin B12 that are coenzymes: the body requires each of them for different reactions.
Cyanocobalamin is the form most commonly found in supplements and fortified foods. It is the most stable because the side group, cyanide, has the strongest attraction to the cobalamin molecule.
Hydroxocobalamin is the form usually contained in B12 shots and the hydroxyl side group has the least attraction to the cobalamin molecule.
Adenosylcobalamin is technically 5′-deoxy-5′-adenosylcobalamin, and also known as dibencozide, cobamamide, and cobinamide.
The coenzyme form of B12 supplements, adenosylcobalamin and methylcobalamin, are sometimes promoted as being superior to cyanocobalamin for two reasons:
Cyanocobalamin contains a molecule of cyanide.
The body must convert cyanocobalamin into adenosylcobalamin and methylcobalamin before using it.
Others suggest that cyanocobalamin is the best choice for most people because it is the most stable form, it has been well studied and proven to increase vitamin B12 status, it is the most common, and least expensive.
Let’s examine the claims in favor of the coenzyme forms.
Cyanide
The safety of cyanocobalamin has raised concerns due to the fact that cyanide is a component of cyanocobalamin. The amount of cyanide in a cyanocobalamin supplement is a fraction of the amount of cyanide most people ingest on a daily basis and is considered to be physiologically insignificant.
For more information, see our detailed analysis in Vitamin B12 and Cyanide.
Effectiveness
[Obeid et al. (2015)] suggest that people do not benefit more from the coenzyme forms because all forms, except injected hydroxocobalamin, must have their side groups stripped by the target cell before the necessary side group is added for the coenzyme form needed. In other words, any form of cobalamin supplement can be turned into both of the coenzyme forms (methylcobalamin and adenosylcobalamin).
They state:
“Currently, we do not have sufficient evidence to suggest that the benefits of using [methylcobalamin] or [adenosylcobalamin] override that of using [cyanocobalamin] or [hydroxocobalamin] in terms of bioavailability, biochemical effects, or clinical efficacy. There is uncertainty regarding the claimed superior role of [B12] coenzyme forms for prevention and treatment of [B12] deficiency. However, [hydroxocobalamin] may be an advantageous precursor of the cofactors, particularly in the inherited disorders of metabolic [cobalamin] processing. [Cyanocobalamin] is a more stable and inexpensive form that appears to be best suited for oral supplementation and parenteral [intravenous] treatment as well.”
People with genetic defects of vitamin B12 metabolism may benefit from hydroxocobalamin injections; Obeid et al. describe these genetic defects in more detail in their paper.
Absorption
Some researchers question whether the coenzyme supplements are stable in their oral form and usually recommend much higher doses of methylcobalamin—typically 1,000 µg/day.
A 1971 study found that at doses of 1 µg, 5 µg, and 25 µg, cyanocobalamin, hydroxocobalamin, methylcobalamin, and adenosylcobalamin were all absorbed at about the same rate [Adams, 1971].
Here’s a table of the absorption rates:
A 1973 study suggests that once absorbed, methylcobalamin may be retained in the body better than cyanocobalamin [Okuda, 1973].
A clinical trial from Korea found that 3 months of 1,500 µg/day of methylcobalamin raised B12 levels, reduced or eliminated neurological symptoms of B12 deficiency, and lowered homocysteine levels [Kim, 2011]. This trial was done on people who had a gastrectomy and, therefore, had vitamin B12 malabsorption, indicating that for most people 1,500 µg/day would be more than enough.
There was no comparison group receiving cyanocobalamin.
I am unaware of any clinical trials testing the various forms of vitamin B12 against each other among the general population and most people seem to do well using cyanocobalamin.
Some people with chronic fatigue report getting more relief from adenosylcobalamin than either methylcobalamin or cyanocobalamin (more info), while other people report feeling better only when taking both adenosylcobalamin and methylcobalamin.
It’s possible this could be a real effect, but could also be due to a placebo effect or taking more B12 and inadvertently counteracting malabsorption.
Methylcobalamin Trial in Vegans
[Donaldson (2000, USA)] studied 3 vegans with elevated urinary MMA levels who were treated with 1/2 to 1 sublingual methylcobalamin tablet, 2 times/day for 3 weeks. Correspondence with the author (March 21, 2002) verified that these tablets contained 1,000 µg methylcobalamin each.
Two of the subjects’ urinary MMA normalized while the remaining subject’s stayed slightly elevated at 4.1 µg/mg creatinine (normal is < 4.0 µg/mg creatinine). Thus, at a rate of 1,000-2,000 µg/day, methylcobalamin appears to be absorbed at a high enough rate to improve B12 status in some vegans. Additionally, this indicates that the methylcobalamin was converted to adenosylcobalamin for use in the MMA pathway.
Cross-sectional Data from Romania
A cross-sectional study from Romania found that vegans supplementing with cyanocobalamin had higher levels of holotranscobalamin than those supplementing with methylcobalamin (150 pmol/l and 78.5 pmol/l, respectively; p-value=0.030; [Zugrav et al, 2021]). However, those taking methylcobalamin supplemented less and the amounts varied.
A holotranscobalamin level of 78.5 pmol/l is well above the minimum healthy range indicating that the methylcobalamin regimen was adequate. The average dose for those supplementing with cyanocobalamin and methylcobalamin was 582 µg and 988 µg, respectively.
The frequency of methylcobalamin intake was 21% daily, 36% twice per week, and 43% once a week. Without assessing MMA levels and more precisely correlating values with intake amounts and frequency it’s not possible to determine a reliable regimen.
Case Study from Germany
[Storz et al. (2024, Germany)] reported a case study of one middle-aged man who had been taking a single oral dose of 500 µg of methylcobalamin and an average of 3 to 4 times a week for many years. His vitamin B12 levels were healthy at 303 pmol/l (409 pg/ml) and his homocysteine level was 11.7 µmol/l (above 12 µmol/l is considered unhealthy).
Anecdotal Report from a Vegan
In 2011, a reader sent in this report:
“I’d been taking 500 µg of methylcobalamin for years, not knowing that the B12 dosages so often cited (daily 25 – 100 µg) are just for cyanocobalamin. So, about a week ago I started taking 1000-2000 µg of methylcobalamin instead of just 500 µg, and I feel a difference!”
It should be noted that this person might suffer from B12 malabsorption of any form of B12, and might have had the same experience with cyanocobalamin.
Hydroxocobalamin
Hydroxocobalamin is the form of B12 typically found in food. There are not many oral forms for people to take; it is normally injected. One study suggests that after injections, hydroxocobalamin is retained in the body better than cyanocobalamin [Tudhope, 1967].
Bibliography
_____________
Chalmers JN, Shinton NK. Comparison of hydroxocobalamin and cyanocobalamin in the treatment of pernicious anaemia. Lancet. 1965 Dec 25;2(7426):1305-8. B12 administered by injection. Not cited.
Donaldson MS. Metabolic vitamin B12 status on a mostly raw vegan diet with follow-up using tablets, nutritional yeast, or probiotic supplements. Ann Nutr Metab. 2000;44(5-6):229-34. The subjects receiving methylcobalamin was only a small part of this paper, mentioned on p. 232.
Kelly G. The co-enzyme forms of vitamin B12: Toward an understanding of their therapeutic potential. Alt Med Rev. 1997;2(6):459-471. Not cited.
Okuda K, Yashima K, Kitazaki T, Takara I. Intestinal absorption and concurrent chemical changes of methylcobalamin. J Lab Clin Med. 1973 Apr;81(4):557-67.
Sawangjit R, Thongphui S, Chaichompu W, Phumart P. Efficacy and Safety of Mecobalamin on Peripheral Neuropathy: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. J Altern Complement Med. 2020 Dec;26(12):1117-1129. Concluded that mecobalamin (aka methylcobalamin) taken orally (1500 mg/day), intramuscularly, or intravenously (500 mg/day) may be effective for the treatment of diabetic neuropathy. Not cited.
Tudhope GR, Swan HT, Spray GH. Patient variation in pernicious anaemia, as shown in a clinical trial of cyanocobalamin, hydroxocobalamin and cyanocobalamin-zinc tannate. Br J Haematol. 1967 Mar;13(2):216-28.





{kind=link}